
Cases with rectal foreign bodies are no longer rare; however, epidemiological data even nowadays are lacking [1]. The first report was published in 1919, although cases have been described since the 16th century [2]. These patients usually present to the emergency department with complains of pelvic or lower abdominal pain [1]. Although there are a wide variety of types of foreign bodies and reasons for insertion, household objects such as bottles or glasses for autoeroticism is one of the most common reasons [2].
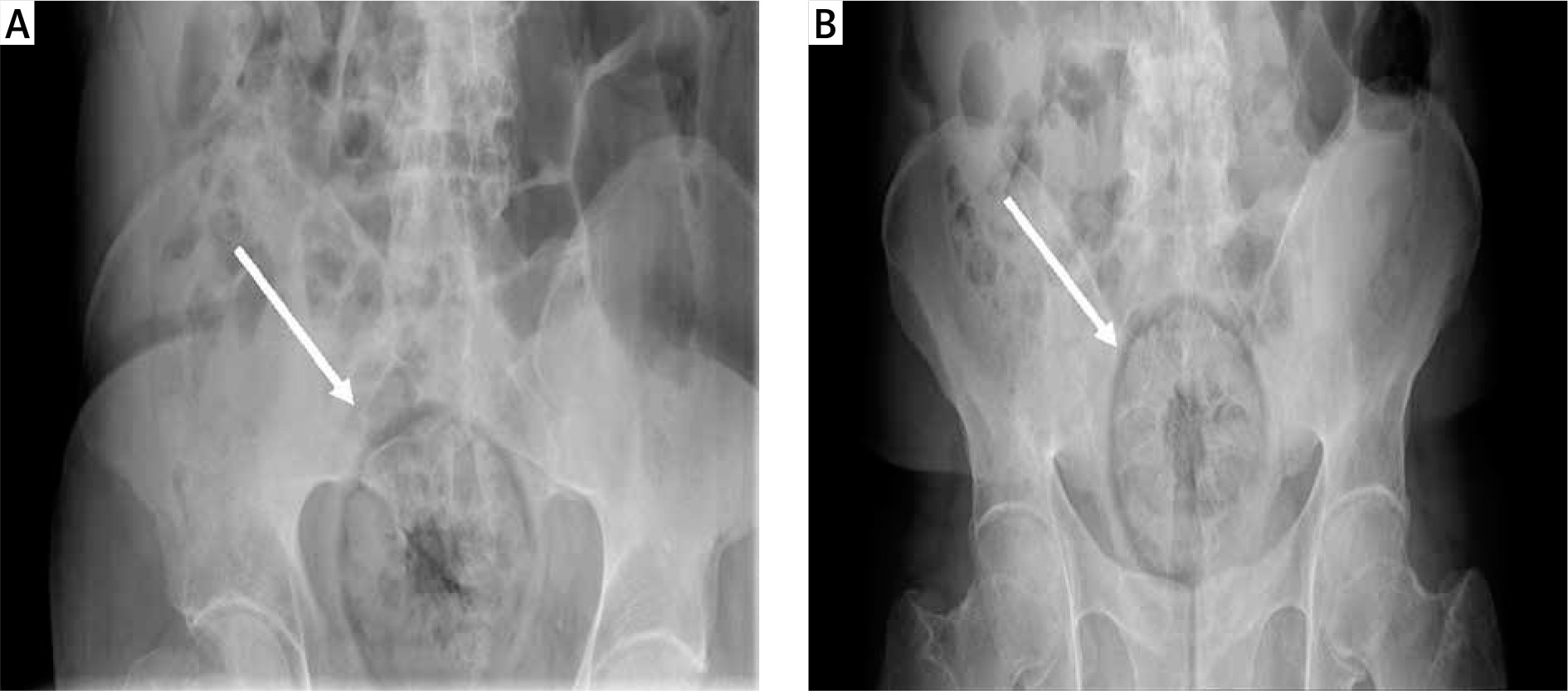
An otherwise healthy 53-year-old male presented to the emergency department with complaints of lower abdominal pain and discomfort from a large round-shaped orange he had inserted in his rectum approximately 12 h prior to presentation. His attempts to remove it at home failed prior to his arrival at the emergency department. On examination, the patient’s temperature was 36.4, heart rate was 85 beats per minute, blood pressure was 138/91 mm Hg, and respiratory rate was 17 breaths per minute. His abdomen was soft and non-distended, and mild tenderness was demonstrated in the left lower quadrant, without signs of peritonitis. The foreign body was palpable in the rectum and no blood was found on the examining glove. His routine blood tests including haemogram, C-reactive protein level, liver, and renal function test were normal. Abdominal radiography revealed a smooth, rounded, radio-dense foreign body within the midline of pelvis (Figures 1 A, B), and there was no evidence of free air.
Figure 1
Abdominal radiograph. A – Supine position, B – erect position. Abdominal radiograph showing a smooth, rounded, radio-dense foreign body within the midline of the pelvis
Because the patient was clinically stable and without evidence of perforation or peritonitis, attempts were made to manually remove the foreign body in the emergency department using anal dilators, forceps and proctoscopy. This was unsuccessful, and as a result of our manoeuvres, the foreign body was pushed higher into the rectum beyond the reach of the examining finger and instrument. The patient was taken to the operating room for examination after anaesthesia and possibly surgical exploration. He was placed in the lithotomy position with reverse Trendelenburg angulation. The surgeon attempted to remove the object manually with lubrication and by using forceps, while suprapubic pressure was applied by an assistant to help move the foreign body. This single trial succeeded, and the foreign body was identified as a 10-cm-long orange (Figure 2). Post extraction, the patient did not have any complications and no abnormality was detected in sigmoidoscopy and abdominal X-ray. He had no abdominal pain and was discharged in a good condition.

Rectal body insertion has been described in the surgical literature since the 16th century [3]. Patients with a retained rectal foreign body are often ashamed of their diagnosis, and it is very important that clinicians speak respectfully with these patients in order to build a trust-based relationship [4]. The good history of the patient and the physical exam including abdominal exam and digital rectal exam are the key points for the diagnosis of such a situation. An abdominal radiograph will confirm the diagnosis [5]. In a stable patient, the foreign body can be extracted in the emergency department transanally with a regional block and/or sedation [6]. Endoscopy can be helpful in cases where the foreign body is located high in the rectum or in the colon [3]. If these fail or the patient is haemodynamically unstable, then he/she should be transported to the operating room for further treatment [3, 7].











