
Pancreatic sinistral portal hypertension (PSPH) is caused by splenic venous outflow tract obstruction, and it accounts for 5% of all cases of portal hypertension [1–3]. When the splenic vein is blocked, the splenic collateral circulation opens, including the short gastric veins (SGVs) and left gastroepiploic vein (LGEV) as the 2 main pathways. The SGVs return to the portal vein through the gastric coronary vein and the LGEV flows through the right gastroepiploic vein to the superior mesenteric vein. Continuous high pressure in the SGVs increases pressure in the gastric mucosal veins, which changes venous structure and results in mucosal varices in the gastric fundus [4, 5]. Gastric variceal bleeding (GVB) is a life-threatening complication of PSPH that requires rapid intervention [6]. Traditional splenectomy is considered the preferred treatment for this condition; however, severe inflammation, adhesions, and bleeding tendency resulting from pancreatitis make the operation difficult and risky. In addition, sepsis and uncontrolled increase in platelet count may occur after the operation [7, 8]. We report herein the success of partial splenic artery embolization (PSAE) in treating a patient with PSPH and associated GVB.
A 50-year-old woman with previous history of chronic pancreatitis presented on 16 July 2012 with persistent upper abdominal distension, nausea, vomiting of gastric contents, and pain of unknown cause. She was diagnosed with acute phase chronic pancreatitis at a local hospital. On 17 August the patient re-presented with melena and haematemesis; gastroscopy revealed ruptured gastric varices with haemorrhage. On 22 August 2012 the patient’s condition deteriorated, and she was transferred to our hospital for treatment. On 23 August the patient underwent abdominal computed tomography (CT; enhancement) and abdominal CT angiography (CTA). This imaging revealed severe acute pancreatitis, a large volume of effusion around the pancreas, local encapsulation, portal vein thrombosis, proximal superior mesenteric vein occlusion, and splenic vein occlusion; pancreatic portal vein hypertension was suspected (Figure 1). During hospitalization, the patient received mechanical ventilation, enteral nutrition, abdominal puncture catheter drainage, and other comprehensive treatments. Her condition gradually improved, and she was transferred to a rehabilitation hospital for further recuperation on 2 November.
Figure 1
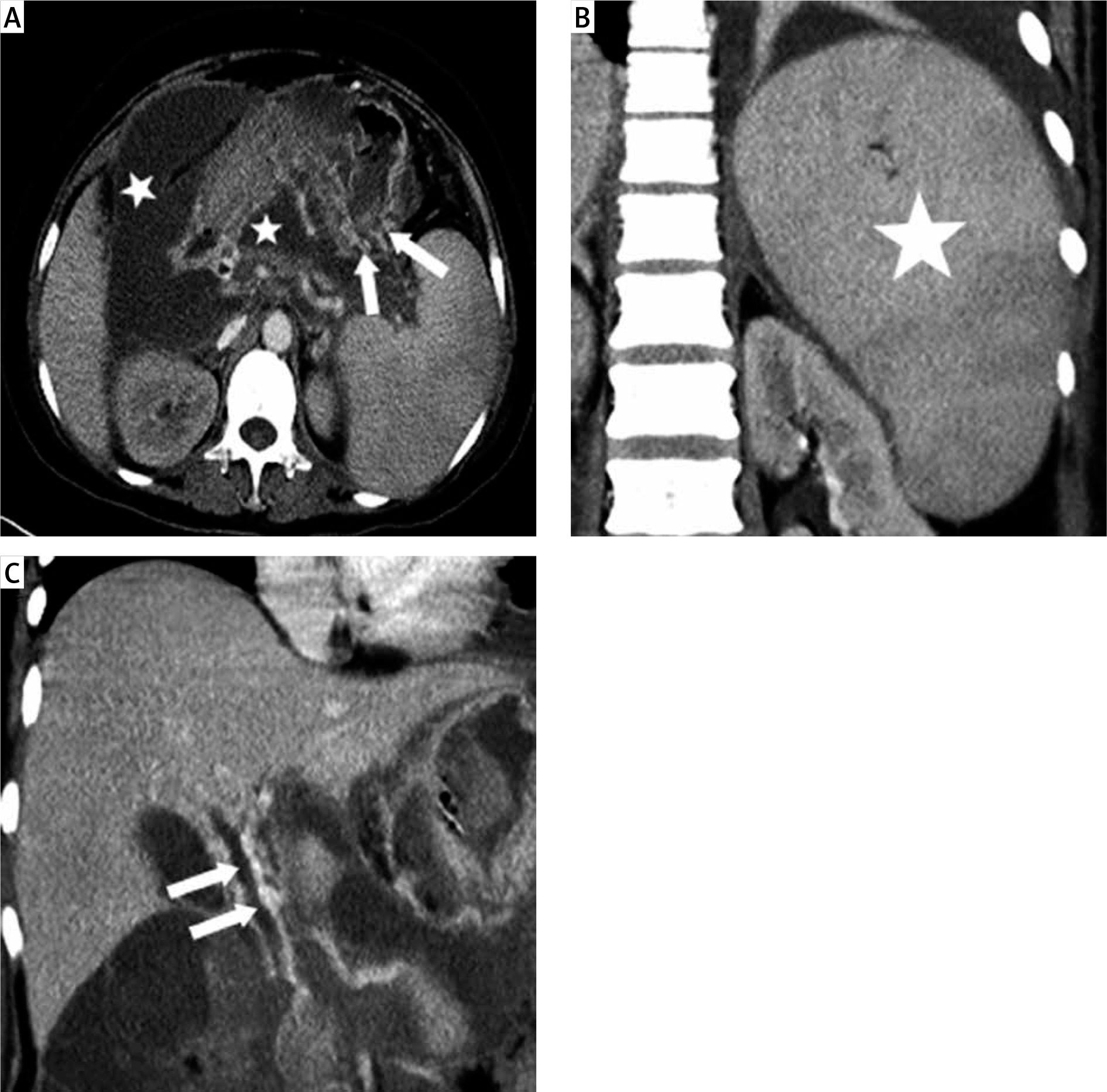
On 22 August 2012 the patient was admitted to our hospital for the first time for complete abdominal CT (enhancement) and complete abdominal CT angiography. A – Veins of the gastric fundus are tortuous and thickened (white arrows), and a large amount of effusion (white stars) is present around the pancreas. B – The spleen is markedly enlarged on coronal views (white stars). C – A filling defect (white arrows) in the portal vein raises suspicion of thrombus formation
Every year during the follow-up period from 2013 to 2018, the patient repeatedly presented with symptoms of melena and haematemesis. She had no previous history of liver cirrhosis. She was diagnosed with PSPH with GVB. Although bleeding resolved each time with conservative treatment, GVB recurred after discharge.
On 6 June 2018 the patient was admitted to our hospital for treatment of melena. Blood test results on that day revealed a haemoglobin (Hb) level of 78 g/l and platelet (PLT) count of 35 × 109/l. Testing on 7 June 2018 revealed Hb of 66 g/l and PLT count of 33 × 109/l, indicating that Hb continued to decrease; the patient had ongoing melena despite conservative treatment at admission. We performed PSAE to treat active GVB on 8 June 2018. Postoperative blood testing on that day revealed Hb of 99 g/L and a PLT count of 41 × 109/l. Hb levels were 105 g/l on 9 June, 108 g/l on 10 June, and 116 g/l on 11 June. PLT count was 46 × 109/l on 9 June, 46 × 109/l on 10 June, and 61 × 109/l on 11 June. The patient had no recurrence of melena after PSAE and was discharged on 12 June 2018. On the day of discharge, repeat whole abdominal CT (enhancement) revealed splenic infarction and no splenic abscess formation but no reduction of gastric varices.
On 29 October 2018 the patient was readmitted to our hospital with melena. Her Hb on that day was 66 g/l and her PLT count was 51 × 109/l. The patient underwent a second PSAE on 31 October. Melena did not recur after PSAE, and her Hb and PLT count gradually returned to normal levels (Figure 2). On 8 November repeat abdominal CT (enhancement) revealed splenic infarction, no splenic abscess formation, and significant regression of gastric varices as compared with images from 7 June 2018 and 12 June 2018 (Figure 3). The patient was discharged from the hospital on 20 November and has had no evidence of GVB recurrence in 38 months of follow-up after discharge.
Figure 2
After the second PSAE, haemoglobin (Hb) and platelet (PLT) values gradually returned to normal. The red line is Hb and the blue line is PLT count
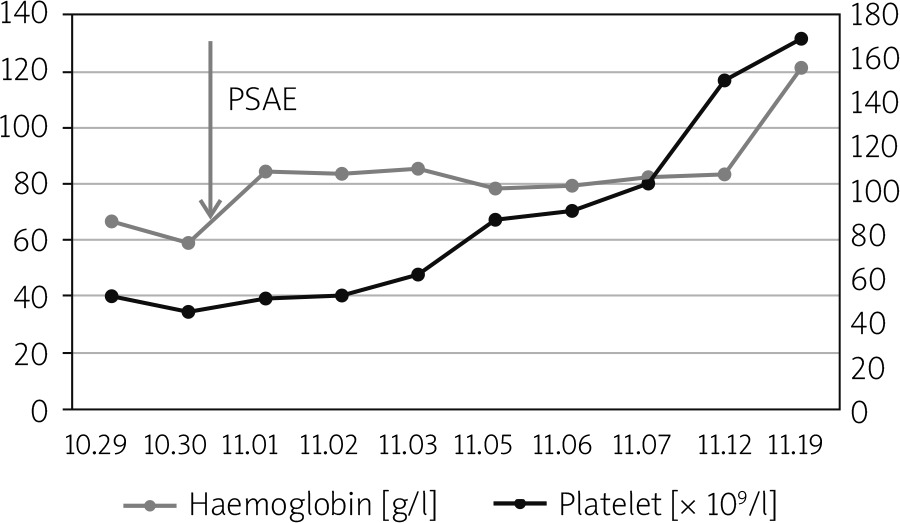
Figure 3
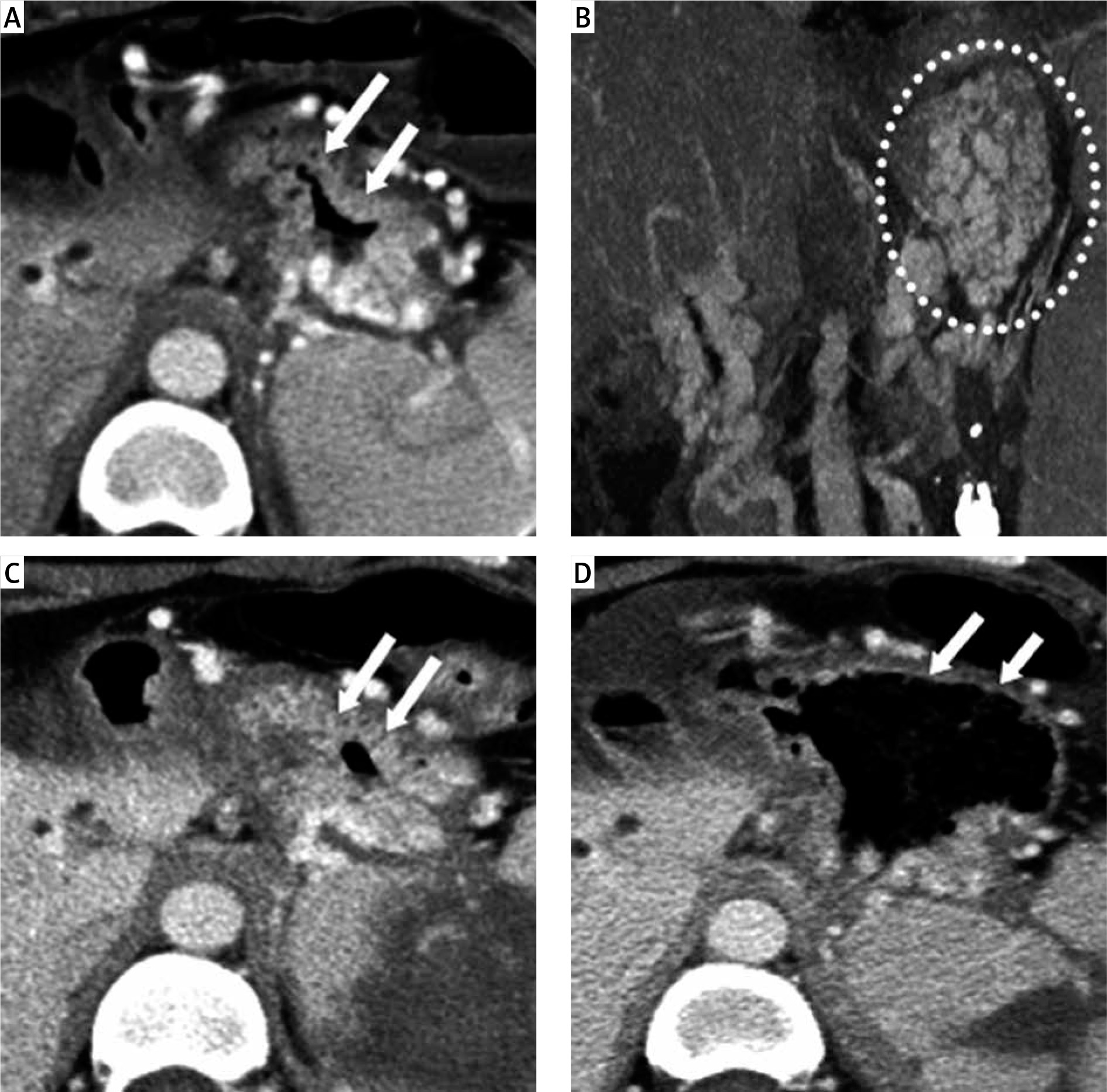
A, B – At the first PSAE, gastric fundus mucosa are thickened (white arrows) and gastric fundus varices (white dotted circle) are seen in the venous phase on enhanced CT. C – After the first PSAE, thickened gastric fundus mucosa (white arrows) are seen in the venous phase on enhanced CT, similar to the findings before the operation. D – After the second PSAE, gastric fundus varices have significantly decreased (white arrows) compared with findings on previous imaging
To prevent postoperative splenic abscess, we prepared the patient with intestinal cleansing before PSAE (oral lactulose, intestinal perfusion with compound lavage solution) and oral administration of norfloxacin capsules on the day before PSAE, the day of PSAE, and the day after PSAE. We used a modified Seldinger technique to puncture the anterior wall of the right femoral artery, insert a 5-Fr catheter sheath (Terumo Corporation, Japan), and insert a 5-Fr RH catheter (Cook, USA) through the sheath tube. The catheter was advanced into the celiac trunk artery for angiography. The arterial phase revealed thickening of the trunk and branches of the splenic artery. Because the patient’s first PSAE had resulted in partial splenic parenchymal infarction, contrast agent staining was not observed in some of the peripheral splenic parenchyma during the parenchymal phase (Figure 4 A). No splenic vein or portal vein development was observed in the venous phase. Next a 2.6-Fr Stride microcatheter (Asahi Corporation, Japan) was advanced into the lower-pole branch of the main splenic artery (Figure 4 B), and an appropriate amount of gelfoam particles (1 cm × 1 cm; Xiangen Medical Technology, China) was injected through the microcatheter. Finally, the microcatheter was withdrawn, and RH catheter angiography revealed that about 40% of the spleen parenchyma did not stain with contrast agent (Figure 4 C). After the operation, the RH catheter and catheter sheath were withdrawn, pressure was applied to the femoral artery puncture point for about 10 min, and then a bandage was applied to the puncture point.
Figure 4
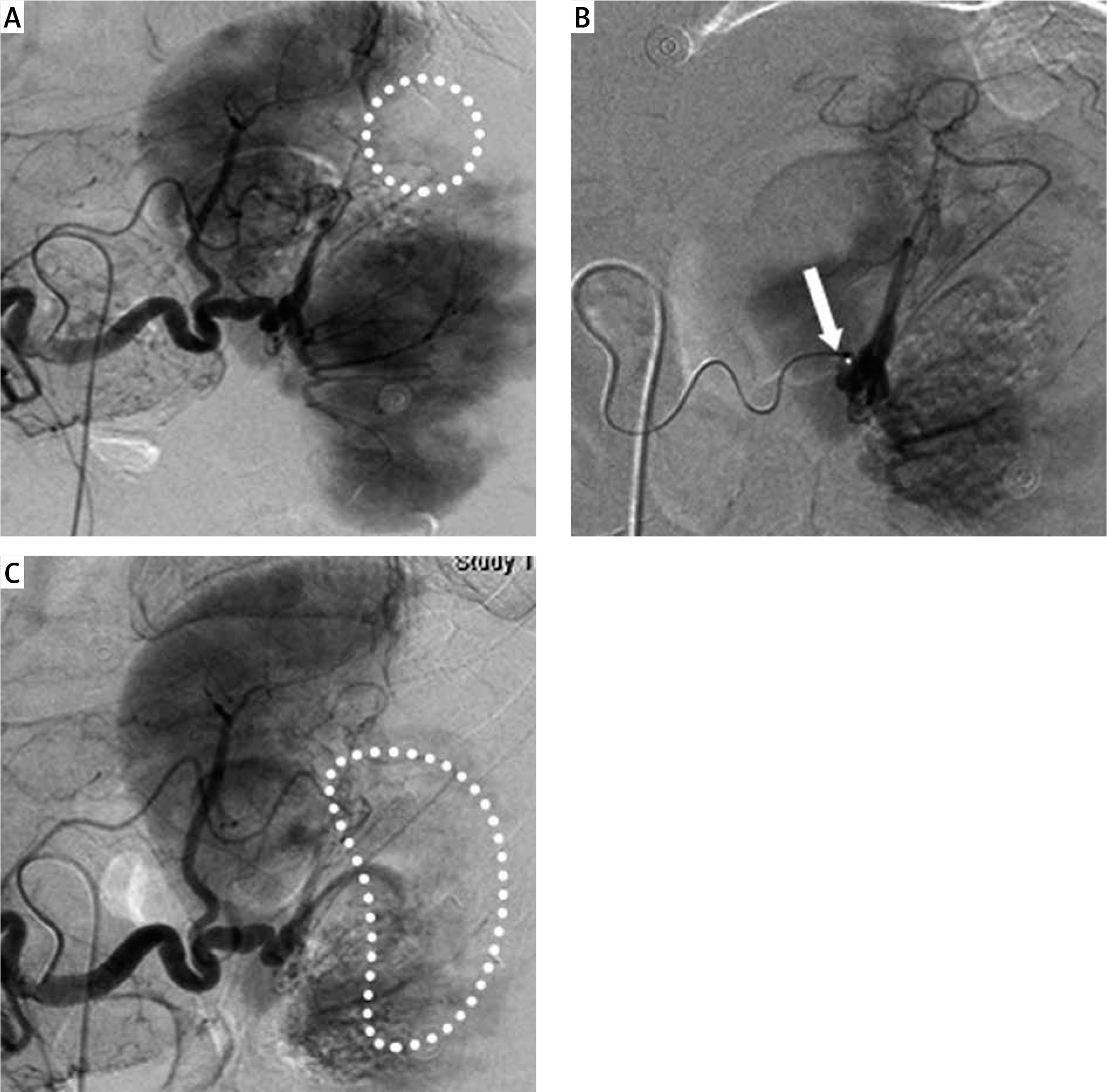
The patient underwent a second PSAE on 31 October 2018. A – Angiography of the splenic artery trunk prior to embolization shows partial absence of contrast agent staining (white dotted circle) in the peripheral splenic parenchyma. B – Superselective microcatheter (white arrow) insertion into the lower-pole branch of the main splenic artery. C – Angiography of the splenic artery trunk after embolization shows new absence of contrast agent staining (white curved dotted circle) in the splenic parenchyma
PSPH differs from cirrhotic portal hypertension in the following ways. First, PSPH patients have no history of liver cirrhosis, and their liver function is normal. Second, isolated gastric fundus varices are present without oesophageal varices. Third, patients have the clinical manifestations of primary pancreatic disease, such as abdominal mass and back pain [2, 9]. The fundamental cause of PSPH is splenic vein outflow obstruction, which has 2 causes: pancreatitis-induced splenic vein thrombosis (PISVT) and extrinsic compression of the splenic vein (splenic aneurysm, pancreatic body and tail tumour, pancreatic pseudocyst and retroperitoneal tumour, retroperitoneal fibrosis, etc.). Of these 2, PIVST is the main cause of PSPH [2].
The reported incidence of PISVT in acute pancreatitis (22.6%) is higher than that in chronic pancreatitis (12.4%) [10]. This difference may be related to the following 2 points. First, the treatment acute pancreatitis requires repeated assessment of the disease, and advances in imaging technology and repeated imaging examination have increased the detection rate of PISVT. Secondly, patients with acute pancreatitis have a high incidence of local complications (peripancreatic inflammatory fluid accumulation, tissue necrosis, abscess, etc.); inflammatory and corrosive fluid around the pancreas stimulates the splenic vein, resulting in severe spastic stenosis of the splenic vein. Encapsulated effusion and abscess may also compress the splenic vein, resulting in splenic vein stenosis.
In the present case, the diagnosis of PSPH was confirmed at the patient’s initial admission to our hospital. First, the patient had no history of liver cirrhosis. Second, she had manifestations of hypersplenism, including decreased PLT and white blood cell counts (41 × 109/l and 3.8 × 109/l, respectively), and the imaging examination suggested splenomegaly. Third, the imaging examination revealed splenic vein compression and occlusion with obvious varices in the gastric fundus, and the patient had a history of GVB prior to hospitalization. However, because of the clinicians’ insufficient awareness of PSPH as a cause of GVB, the patient was not treated radically.
The incidence of GVB as a complication of PSPH is 12.3% [10], and it requires immediate treatment once it occurs. Conservative treatment has short-term haemostatic effects; however, GVB will recur and radical treatment on the basis of conservative treatment is necessary.
The traditional complete splenectomy can completely cut off all blood flow to the spleen, reduce the flow through the SGV, significantly reduce the pressure in varices in the gastric fundus, and achieve haemostasis [11, 12]. However, splenectomy has several disadvantages. First, complete splenectomy results in complete loss of spleen function, with postoperative hard-to-control thrombocytopaenia and decreased immunity. Second, high levels of free trypsin in the abdominal cavity of patients with pancreatitis can corrode the abdominal blood vessels, leading to a high risk of death from massive haemorrhage during splenectomy. Third, pancreatitis causes an inflammatory cascade in the abdominal cavity with diffuse inflammatory effusion, resulting in extensive adhesions and fibrosis of the abdominal vessels and tissues, which can obstruct the surgeon’s view and complicate dissection of the splenic artery. Fourth, patients with pancreatitis often have associated abdominal infections, and splenectomy increases the risk of postoperative sepsis [7, 8]. In recent years, laparoscopic splenectomy has been used to treat haematological diseases because of its minimally invasive nature and feasibility; however, there have been no reports of laparoscopic splenectomy in patients with PSPH and GVB [13, 14].
To reduce blood flow into the spleen while retaining splenic function, surgeons developed the Warshaw operation. In this procedure, the main splenic artery is severed, and 2 sets of collateral arteries – the short gastric arteries (SGAs) and the LGEA – are retained to supply blood to the spleen [15, 16]. However, the application of this procedure in PSPH with GVB is limited. Although gastric varices improve in the short term due to the decreased blood flow into the spleen, over time the compensatory blood flow via the SGAs and LGEA gradually increases, leading to increased pressure in the SGVs and recurrence of GVB [17].
With the development of interventional radiology, PSPH with GVB is increasingly treated with endovascular treatment instead of surgery. Splenic artery embolization is called “non-surgical splenectomy” and is divided into PSAE and total splenic artery embolization (TSAE) [18–20]. PSAE, also known as distal embolization, is the injection of a pellet embolization agent through a catheter to embolize a graded branch or multistage branch of the main trunk of the splenic artery. This procedure is mainly used in patients with hypersplenism and in those with GVB caused by liver cirrhosis. In 1973, Maddison [21] first used transcatheter embolization of the spleen instead of surgical splenectomy to treat a patient with advanced cirrhosis who had haemorrhage from esophagogastric fundal vein rupture. Shimizu et al. [22] found that after PSAE, blood flow from the splenic vein to the portal vein significantly decreased, thereby reducing portal vein pressure and reducing the risk of bleeding from the rupture of oesophageal and gastric varices caused by liver cirrhosis.
The patient in the current study repeatedly presented over many years with GVB caused by PSPH. These recurrences seriously affected her quality of life, and finally we decided to treat her with PSAE. After the first PSAE, the patient’s PLT count before discharge was slightly higher than on admission, but it was still low (61 × 109/l). The recurrence of GVB 4 months after discharge was considered to be related to an insufficient degree of PSAE at the initial treatment. After the second PSAE, the degree of varicose veins in the gastric fundus decreased significantly, the PLT count returned to normal (169 × 109/l), and no GVB occurred in 38 months of follow-up after the second discharge.
TSAE, also known as proximal embolization, is the injection of an embolization agent into the trunk of the splenic artery at the splenic hilum to completely embolize the trunk of the splenic artery. TSAE is more suitable than PSAE for blunt splenic injury for 2 reasons. First, after embolization of the main splenic artery, the potential collateral arteries (SGAs and LGEA) open to supply the residual splenic parenchyma, thus preserving some splenic function, an effect similar to that of the Warshaw procedure. Second, blood flow in the internal splenic artery is blocked, which is conducive to the formation of thrombosis, making multiple arterial injuries and bleeding in the spleen easy to control [23–25]. However, TSAE alone may not be a good choice in the treatment of PSPH with GVB because, with the increase in compensatory collateral circulation, there is an ongoing risk of re-rupture and bleeding from gastric varices [17].
Metal coils, polyvinyl alcohol (PVA) particles, and gelatine sponge particles are the most common embolization agents for SAE [26–29]. Metal coils are most commonly used in TSAE for the treatment of blunt splenic injury, whereas PVA particles and gelfoam particles are most commonly used in PSAE [23, 25]. We chose gelatine sponge particles for PSAE embolization for 2 reasons [30]. First, PVA particles will cause more severe splenic infarction and inflammatory exudation than gelatine sponge particles, resulting in increased splenic capsule effusion and capsule tension, severe postoperative pain, and even a risk of splenic rupture. Second, the thrombogenesis induced by gelatine sponge particles does not depend on the patient’s coagulation state. Patients with PSPH have very low PLT counts and coagulation function is compromised, so gelatine sponge particles are more suitable than PVA particles for embolization in patients with PSPH and GVB .
GVB is a lethal complication in patients with PSPH, and it requires urgent intervention. PSAE is an effective and minimally invasive method for the treatment of PSPH with GVB.










