
Introduction
Gastric cancer (GC) is ranked fourth in all cancers and second in cancer-related deaths worldwide [1]. It is 2–3-times more common in males than in females. The highest incidence is in the Far East, Eastern Europe, and South America, and the lowest incidence is in the majority of North America and Africa [2].
Genetic and environmental factors play a role in GC development. Studies have shown an association between gastrointestinal system cancers and inflammation. Helicobacter pylori, smoking, alcohol, and obesity are the main causes of inflammation in gastric mucosa [3, 4]. Gastritis leads to the activation of neutrophils, lymphocytes, macrophages, and platelets. Long-term inflammation leads to multistage histopathological changes called Correa tract, which includes gastritis, atrophy, intestinal metaplasia (IM), dysplasia, and cancer stages [5].
Because the patients are generally symptomatic in advanced stages, diagnosis is usually delayed. Endoscopic screening of patients with nonspecific symptoms in areas with low incidence of gastric cancer is not cost-effective and is invasive. Early diagnosis is lifesaving in these patients as well [6]. It is essential to diagnose the disease with low cost blood tests when curative treatment can be performed [7]. Neutrophils and lymphocytes in the tumour microenvironment constitute a large part of the tumour stroma [8]. The role of activated platelets in cancer development and metastasis has been established [9]. In previous studies, some haematological parameters such as mean platelet volume (MPV), neutrophil lymphocyte ratio (NLR), platelet lymphocyte ratio (PLR), and red cell distribution width (RDW) have been associated with tumour development, progression, and survival [10–12].
Aim
The aim of our study is to determine if there is any difference in haematological parameters such as NLR, PLR, MPV, RDW, plateletcrit (PCT) and platelet distribution width (PDW) between patients with GC, IM, and healthy controls (HC).
Material and methods
Between January 2014 and January 2017, 73 patients with histopathologically proven GC (adenocarcinoma), 79 patients with IM (according to Sydney Classification, at least one histopathological +++ IM from antrum or corpus), and 70 HCs were included this retrospective study at the Gastroenterology Clinic of Kecioren Training and Research Hospital. Patients with hypertension, diabetes mellitus, antiplatelet drug use, hyperlipidaemia, thyroid diseases, autoimmune diseases, rheumatological diseases, heart failure, chronic liver disease, chronic renal diseases, and patients with previous cancer were excluded from the study.
Demographic characteristics and laboratory parameters of complete blood count were obtained from the hospital medical database records. The evaluation of blood parameters was performed within one hour of venepuncture by Siemens Healthcare Diagnostic Item ADVIA 2120i.
In our laboratory, normal values for studied blood parameters ranged as follows: platelet: 142–424 × 103/μl, MPV: 7.8–11 fl, RDW: 11.6–17.2%, white blood cells (WBC): 4.6–10.2 × 103/μl, neutrophil: 2.0–6.9 × 103/μl, lymphocyte: 0.6–3.4 × 103/μl, monocyte: < 0.9 × 103/μl, PCT: 0.15–0.62%, PDW: 8.3–25 fl.
Statistical analysis
Statistical analysis was performed with the SPSS software (SPSS 15.0, Chicago, IL). The optimal cut-off values of NLR and PLR were estimated by the receiver operating characteristics (ROC) curve. The area under the curve (AUC), sensitivity, and specificity were calculated. Continuous variables were expressed using mean ± SD. Comparisons between groups were performed using χ2 test. P-values < 0.05 were defined as significant.
Results
Seventy-three patients with new GC, 79 patients with IM, and 70 HC were enrolled in the study. The demographic data and complete blood parameters of patients and control group are shown in Table I. There was no statistically significant difference in terms of age and gender between groups.
Table I
Demographic characteristics and laboratory parameters of patients
| Parameter | GC (n = 73) | IM (n = 79) | HC (n = 70) | P-value |
|---|---|---|---|---|
| Age [year] | 67.1 ±11.1 | 65.1 ±10.8 | 65.3 ±10.0 | 0.468 |
| Gender, male (%) | 35 (47.9) | 43 (54.4) | 38 (54.3) | 0.667 |
| Hb [g/dl] | 11.4 ±2.1 | 13.4 ±1.9 | 14.2 ±1.1 | < 0.001a |
| RDW (%) | 17.3 ±4.1 | 16.0 ±3.1 | 14.4 ±1.4 | < 0.001b |
| WBC [× 103/μl] | 8.27 ±2.90 | 6.78 ±1.61 | 6.96 ±1.15 | < 0.001c |
| Platelet [× 103/μl] | 299.3 ±141.3 | 236.3 ±62.0 | 249.4 ±53.2 | <0.001d |
| MPV [fl] | 7.59 ±1.03 | 7.69 ±1.27 | 8.15 ±0.88 | 0.007e |
| PDW [fl] | 17.4 ±1.8 | 17.8 ±1.1 | 16.0 ±1.9 | < 0.001f |
| NLR | 3.18 ±2.14 | 1.94 ±1.07 | 2.15 ±1.11 | < 0.001g |
| PLR | 173.7 ±104.2 | 116.0 ±48.8 | 127.4 ±54.9 | < 0.001h |
| MLR | 0.35 ±0.018 | 0.26 ±0.16 | 0.24 ±0.11 | < 0.001i |
GC – gastric cancer, IM – intestinal metaplasia, HC – healthy control, RDW – red cell distribution width, WBC – white blood cells, MPV – mean platelet volume, PDW – platelet distribution width, NLR – neutrophil-to-lymphocyte ratio, PLR – platelet-to-lymphocyte ratio, MLR – monocyte-to-lymphocyte ratio.
The mean Hb levels were statistically significant between all three groups. Mean RDW, WBC, MPV, PDW, NLR, PLR, and monocyte-to-lymphocyte (MLR) levels were statistically significantly different between gastric cancer and healthy control groups. Mean RDW, MPV, and PDW levels were statistically significantly different between IM and healthy control groups. Mean WBC, NLR, PLR, and MLR levels were statistically significantly different between gastric cancer and IM groups.
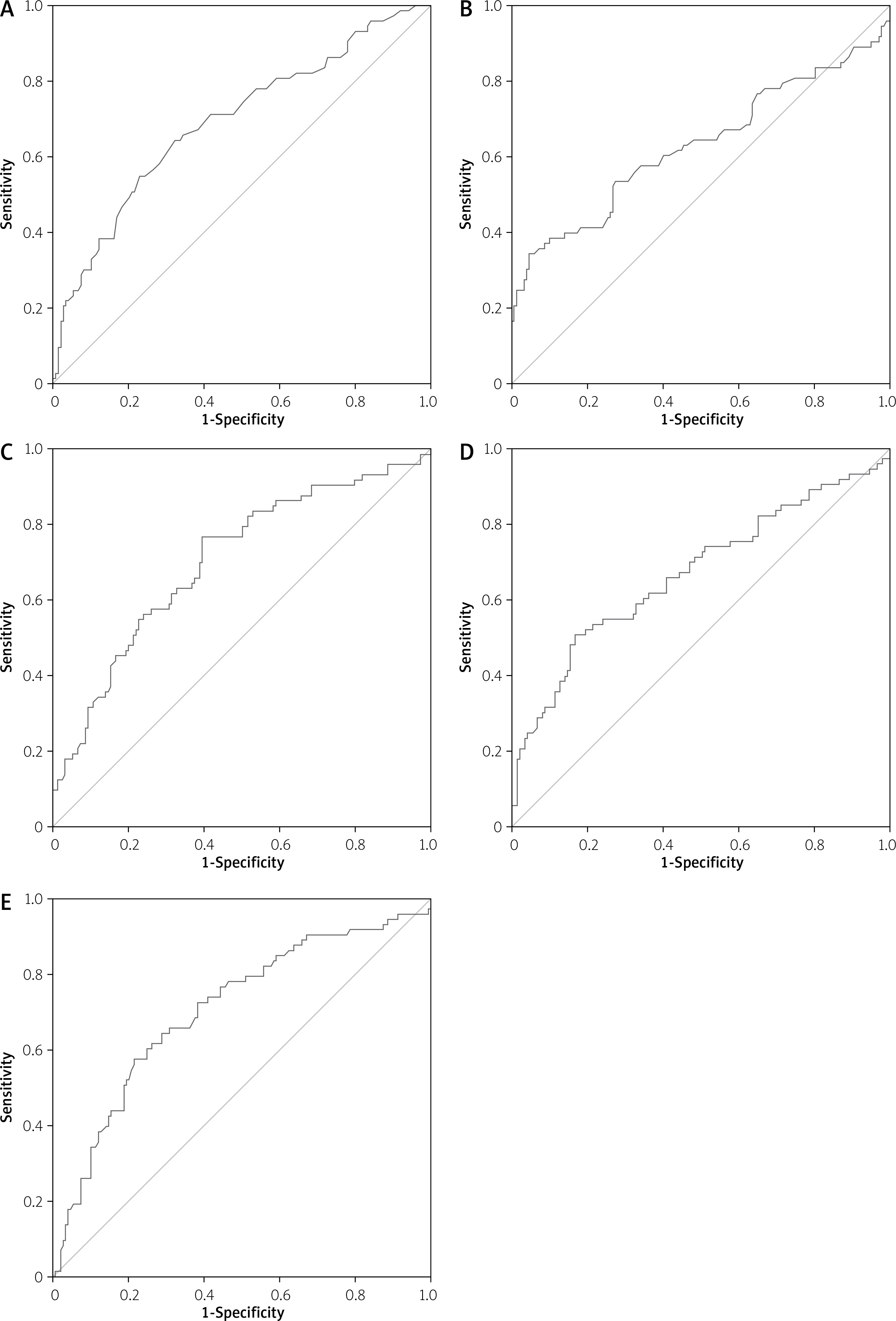
ROC analysis (Figure 1, Table II) showed the ideal platelet cut-off value was 249 × 103/μl (AUC = 0.63, sensitivity: 60.3%, specificity: 59.7%) and 15.55 as the cut-off value of RDW (AUC = 0.70, sensitivity: 65.8%, specificity: 65.8%) and 2.11 as the cut-off value of NLR (AUC = 0.70, sensitivity: 64.4%, specificity: 63.1%) and 124.9 as the cut-off value of PLR (AUC = 0.67, sensitivity: 61.6%, specificity: 63.8%) and 0.27 as the cut-off value of MLR (AUC = 0.71, sensitivity: 65.8%, specificity: 69.1%).
Table II
Cut-off value of RDW, platelet, NLR, PLR, and MLR between the gastric cancer and intestinal metaplasia groups
Discussion
GC is one of the cancer types with high mortality rates, and early diagnosis is principal in decreasing these rates [7]. The relative risk of progression GC from IM is up to 30-fold. Previous studies have examined if there is a differential role of various inflammatory markers such as NLR, PLR, MPV, and platelet counts in patients with gastric cancer and healthy controls [10–13]. However, to our knowledge there is no study with these inflammatory markers to distinguish patients with GC and IM, and HCs.
In our study there was a significant difference in terms of all parameters between patients with GC and HCs. There was no significant difference in terms of RDW, MPV, and PDW between patients with GC and IM. Also, there was a significant difference in terms of Hb, WBC, platelet, NLR, PLR, and MLR between patients with GC and IM. There was no significant difference in terms of WBC, platelet, NLR, PLR, and MLR between patients with IM and HC, and there was a significant difference in terms of Hb, RDW, MPV, and PDW between patients with IM and HC.
Increased platelet counts were seen in gastrointestinal cancers, which has been associated with poor prognosis and shorter survival rates. It is thought that the high number of platelets in the cancer is due to activation of the thrombocytosis pathway because of the cytokines released from the tumour tissue [14]. In our study the platelet count was significantly higher in the GC group than in the IM and HC groups, but there was no significant difference between IM and HC. MPV is an early index of activated platelets. Yun et al. stated that MPV can be a possible biomarker in the diagnosis and follow-up of GC independently of tumoural stage. In a study from China decreased levels of MPV were found in gastric cancer patients compared to gastric ulcer patients [15]. We found lower levels of MPV in the GC and IM groups than HC, which is in contrast to the study of Kılınçalp et al. The reason of the diversity in terms of platelet count and MPV levels between GC, IM, and HC groups is unclear. Also, low levels of MPV in gallbladder cancer and locally advanced oesophageal squamous cell carcinoma have been reported recently [16, 17]. Decreased MPV may be related with consumption of large platelets in inflammatory states [18]. PDW is the measurement of platelet cell volume with flow cytometry, and it is an indicator of platelet activation [19]. We found significantly lower PDW levels in GC and IM patients than HC, as reported before [20]. However, RDW is a parameter of iron deficiency anaemia, and it has been suggested that it can be used as a diagnostic or prognostic marker of various cancer types [21, 22]. It is thought that the increase in inflammation causing carcinogenesis supresses erythropoietin secretion and leads to a decrease in iron release from the reticuloendothelial system and consequently a decrease in erythrocyte life and an increase in RDW [23]. Our findings were comparable with the study previously reported [20].
Neutrophils, lymphocytes, platelets, and monocytes are components of tumour-induced systemic inflammatory response (SIR). Lymphocytes have an antitumour effect, and neutrophils secrete cytokines and chemokines that induce tumour progression and metastasis. Platelets can accelerate tumour growth by secreting angiogenetic factors and pro-inflammatory cytokines. Macrophages derived from monocytes that phagocytes tumour cells [8, 9, 24, 25]. Pietrzyk et al. reported that platelet count, MPV, RDW, NLR, and PLR can be used to discriminate GC patients from HCs [12]. Chen et al. reported that MLR predicts survival in patients with advanced GC undergoing neoadjuvant chemotherapy [26]. Song et al. reported that MLR may be a better biomarker for predicting overall survival of patients with advanced gastric cancer [27]. Our results were similar to these previous studies. Being a single-centre retrospective study and including a small number of patients are the limitations of our study.











