
Introduction
Inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis, (UC) are chronic, inflammatory disorders of unknown aetiology involving the gastrointestinal tract. The most common symptoms of IBD encompass diarrhoea, abdominal pain, and weight loss; however, clinical manifestations can be very heterogeneous, depending on the disease location and phenotype [1]. Many patients receive aggressive immunosuppressive drugs in order to achieve clinical and endoscopic remission. Nevertheless, a significant number of patients require surgical treatment due to lack of response to pharmacological therapy or as a result of severe complications [1].
The prevalence of IBD is increasing worldwide in developed countries [2]. These epidemiological tendencies are also observed in Poland; however, there are no long-term Polish prospective data on IBD incidence. According to the Polish registry of CD, the number of CD patients exceeds 7000, but it is believed that these data are underestimated. According to the estimations of the Polish Gastroenterological Association, there are 10,000–15,000 CD and 35,000–40,000 UC patients in Poland, and these numbers are increasing [3]. Because both CD and UC concern mainly young patients, IBD has become a significant problem also from a sociological point of view in recent years. The disease burden has an influence on many aspects of the patient’s functioning and decreases their overall quality of life [4]. In order to assess these phenomena objectively, an IBD Disability Index (IBD-DI) has been proposed [5]. This is a validated tool, which can help clinicians to guide different therapeutic decisions. Nevertheless, due to its complexity it is difficult to use it in everyday clinical practice. Lately, a simplified version of the IBD-DI has been developed: the IBD Disk [6]. This tool assesses the following 10 items: abdominal pain, body image, education and work, emotions, energy, interpersonal interactions, joint pain, regulating defecation, sexual functions, and sleep. The final version of the IBD Disk was created in a multistep consensus process and it is based on the similar Psodisk platform, which was developed for patients with psoriasis. It can be used in an outpatient setting, also as a mobile application, to give an immediate visual representation of patient-reported, IBD-related disability [6].
Material and methods
The idea of the Polish adaptation of the IBD Disk arose during IBD Preceptorship in Birmingham in June 2018 (Subrata Ghosh, Piotr Eder). After the acceptance of Prof. Subrata Ghosh, the next steps were taken. In cooperation with the President of the Polish Gastroenterological Association, a working group was selected from Polish specialists in gastroenterology and IBD (Piotr Eder, Michał Łodyga, Ariel Liebert, Maria Kłopocka, Magdalena Kaniewska, Agnieszka Dobrowolska, Grażyna Rydzewska).
The IBD Disk is a 10-item visual instrument, which can be used also as a mobile application or application for personal computer (Figure 1). For each of the questions related to 10 categories, the patient should score his or her level of agreement on a scale of 0 to 10, where 0 means “absolutely disagree” and 10 means “absolutely agree” (Table I). In the next step the patient should circle all the scores on a coloured disc, which gives the final graphic visualisation of the current disability burden of the disease [6].
Figure 1
The IBD Disk visualisation. The circle contains 10 items related to disability, which are assessed by the patient (Source: Ghosh et al. Inflamm Bowel Dis 2017; 23: 333-40). See details in the text
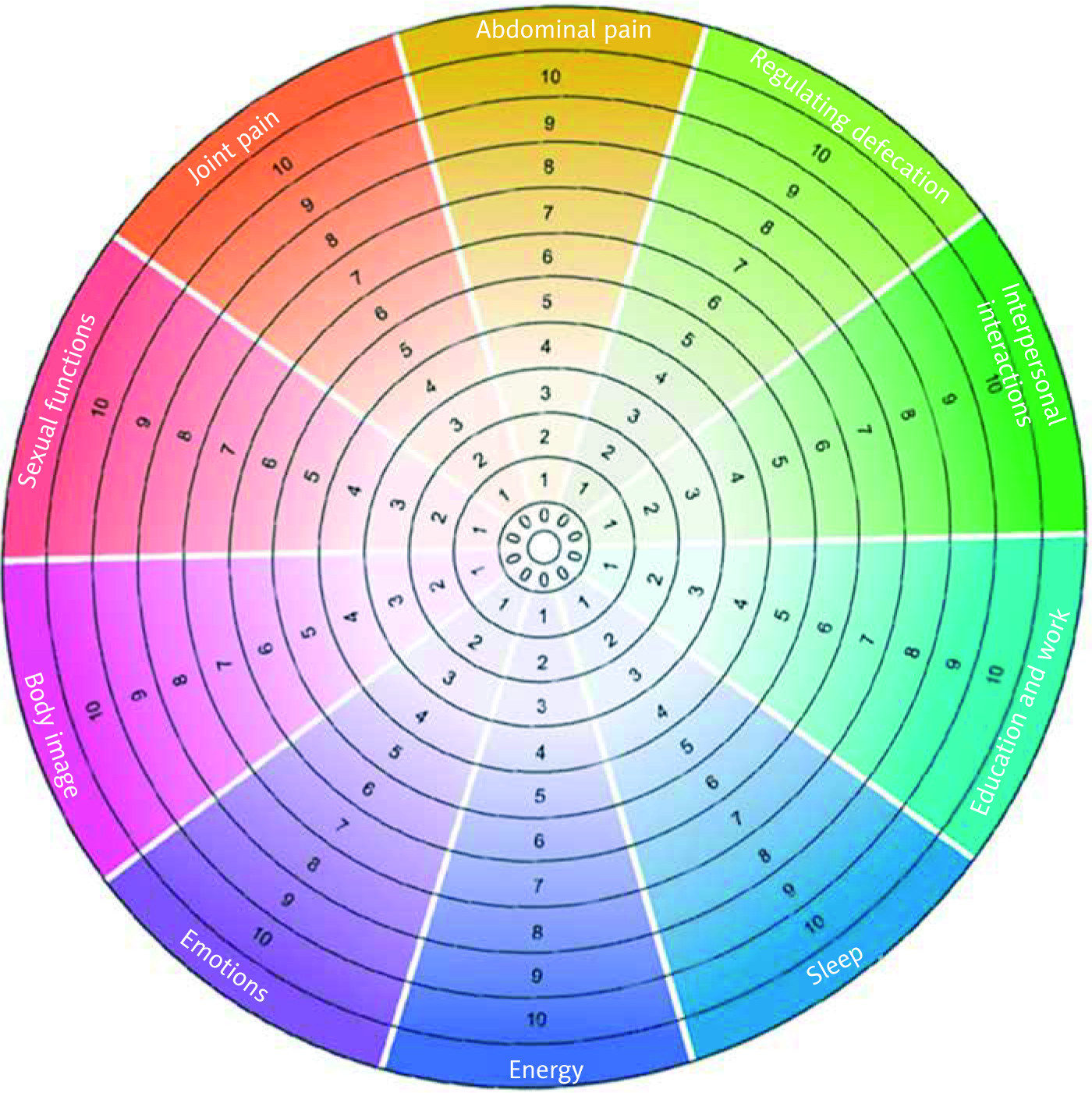
Table I
The table presents questions from the original English version of the IBD Disk and its final Polish translation
In order to adapt the IBD Disk for Polish doctors and patients, a multistep process was initiated. In the first step the English version of the IBD Disk was translated into Polish language, separately, by the members of the working group and by a professional translation agency (the translation phase). Then, after comparing and discussing all translations, the working group accepted in an on-line manner the final version after full agreement was achieved. In the next step, re-translation of the Polish IBD Disk version into English language was conducted by a professional translation agency (the re-translation phase). Then, the concordance of the re-translated version with the original one was assessed by the members of the working group. After full agreement was achieved, the final Polish version was accepted. In the last step the Polish IBD Disk version was sent to 10 persons (nurses, dietitians, students) in order to assess the understandability of the items used in the application. Moreover, 50 consecutive IBD patients were asked to rate the ease of use of the tool in a semiquantitative scale from 1 to 10, where 1 means “very easy” and 10 means “very difficult”.
Results
In the initial translation phase, the concordance between translation agency and experts was very high. There was only some discrepancy concerning the term “Sexual functions”, because a direct Polish translation seems not to be suitable and does not reflect the original meaning of this item. We were considering two options referring more to “Sexual activity” or “Sexual functioning”, finally accepting the Polish version “Funkcjonowanie seksualne”.
In the re-translation phase only some stylistic and grammatical corrections were made. In the final step the general assessment of understandability of all items was high. Moreover, patients with IBD assessed the ease of use of the IBD Disk as very easy (median: 1.5 points, 95% confidence interval: 1.0–2.0).
Table I presents the questions related to the 10 main items of the IBD Disk in the original English version and in the final Polish version.
Discussion
The current approach to the care of patients with IBD should take into account not only the assessment of clinical symptoms and disease activity by using serological markers, endoscopic, and radiological methods, but also it should consider the influence of IBD on patients’ everyday activity and functioning [7]. There are many data showing that active IBD can decrease the overall quality of life [4–6]. A significant proportion of patients develop anxiety and depression, which can also deteriorate the course of IBD [8]. Body image and self-acceptance are impaired, and the disease burden can result in sleep disturbances, can alter the ability to work, hinder everyday household activities, and limit educational opportunities [6, 9–12]. Moreover, IBD can lead to difficulties with personal relationships and participation in community, and very often it impairs sexual functions [6, 13]. All of these phenomena worsen the everyday functioning of patients with IBD and cause disability.
Because clinicians were lacking a reliable tool assessing disability in IBD, a dedicated and validated tool for this purpose was proposed – the IBD-DI [5]. The published version of this questionnaire comprises 28 items covering different aspects of disability [5, 6]. A modified version of the IBD-DI was also released, comprising 14 disability-related questions [14]. Nevertheless, using the IBD-DI can be time-consuming, and due to its complexity, it is difficult to use it more commonly in everyday clinical practice. The IBD Disk is a simplified version of the IBD-DI and was created in a sophisticated, methodological, multistep process in order to allow clinicians and patients to carry out practical implementation of routine assessment of disability in IBD [6]. The IBD Disk is aimed not only to dynamically assess the influence of chronic disease on different aspects of patients’ life, but it also has the potential to help gastroenterologists to guide clinical decisions together with a patient. This holistic approach enables the estimation of a total disease activity/burden and is an example of a participatory medicine, in which the patient is actively engaged in medical care at all stages of the disease [6].
The main aim of adapting the IBD Disk in Poland was to improve the quality of care of Polish IBD patients. For several administrative reasons, the situation of this group of patients is difficult [15]. The reimbursement and practical introduction of the newest therapeutic molecules (ustekinumab, vedolizumab) are delayed in Poland. The possibilities for optimal use of anti-TNF agents are increasing, but the maximum time period of the therapy is still only 2 years for CD and 1 year in the case of UC. The number of physicians in Poland is among the lowest in Europe [16]. Thus, access to specialist medical care is difficult. On the other hand, Poland belongs to the most dynamically developing countries in Europe, with the lowest unemployment rates and the best economic ratings. The computerisation of Polish society and access to the latest technological achievements is vast. Moreover, Polish patients – especially at younger age, like those with IBD – are aware of their rights and want to actively participate in different pro-health initiatives by using media and mobile applications [17]. Polish associations supporting people with IBD are very active, and they support every opportunity to increase the social awareness of administrative and medical problems of this group of patients. Thus, introduction of the IBD Disk as a mobile application in Poland can improve the communication between gastroenterologists and patients, allowing better access to medical care. This could also be an opportunity to promote knowledge on IBD in Poland.
Conclusions
We performed a multistep adaptation process of the IBD Disk in Poland in order to offer a new scientific and clinical tool directly reflecting the original version.
The next step for the IBD Disk in Poland, after launching the final version of this tool, will be to validate it in different cohorts of patients by comparing it with other well-known indices and scales, like the IBD-DI, IBD-Questionnaire, Work Productivity and Activity Impairment Questionnaire: General Health (WPAI-GH) instrument, patient-based Simple Clinical Colitis Activity Index (p-SCCAI), and others in longitudinal, prospective, multicentre trials [18, 19]. This step is crucial because the operating characteristics of the IBD Disk in clinical practice as an outpatient tool have not been fully validated [6]. All of those steps will be performed in strict cooperation with the Institute of Translational Medicine at the University of Birmingham. Then we plan to promote the use of the IBD Disk in everyday clinical practice among Polish gastroenterologists and Polish IBD patients in order to improve the quality of care in IBD in Poland.











