
Introduction
Van Wyk-Grumbach syndrome (VWGS) is a rare condition characterized by severe hypothyroidism with symptoms of incomplete isosexual precocious puberty (PP). As hypothyroidism is a common condition in children, only a severe case can cause the occurrence of VWGS.
The pathophysiology of this syndrome shows the incredible complexity of the hormonal axes. In primary hypothyroidism, we observe reduced levels of free thyroid hormones (even indeterminate), elevated thyroid stimulating hormone (TSH), and thyrotropin-releasing hormone (TRH) levels. As a glycoprotein, TSH is structurally similar to follicle-stimulating hormone (FSH). Therefore, high levels of TSH can cause a situation where a TSH molecule interacts with the FSH receptor in the ovaries [1–3]. Their stimulation leads to an increase in the estradiol levels, causing the development of PP, metrorrhagia, and multiple follicles in the ovaries (even cysts) without the development of axillary and pubic hair in the absence of adrenarche [1]. Luteinizing hormone (LH) is also similar to FSH. Still, elevated levels of this hormone are not observed due to the inhibiting influence of prolactin, higher levels of which are induced by elevated levels of TRH [4]. Prolactin also increases the ovaries’ sensitivity to circulating gonadotropins and promotes follicular maturation [2, 4, 5]. In boys, elevated FSH levels and prepubertal LH levels lead to testicular enlargement without Leydig cells’ stimulation and, therefore, also without increased levels of testosterone [6]. In girls, usually, breast development and vaginal bleeding are observed. Ultrasonography shows a pubertal uterus and ovarian cysts [3]. Sometimes, due to increased levels of prolactin, galactorrhoea occurs [1]. Boys experience macroorchidism. Both girls and boys do not have signs of virilization. Their bone age and growth are delayed, which can be the main difference between VWGS and gonadotropin-releasing hormone (GnRH)-dependent PP [3, 4]. VWGS is a rare disorder [7]. According to the analysis conducted by Fernandez-Gonzalez et al., the median age at diagnosis of VWGS is 8.75 years, and this syndrome is diagnosed more often in girls [1]. The treatment of this syndrome is the administration of a synthetic form of thyroid hormone; for this treatment, almost every patient with this syndrome responds well [1, 8]. The clinical symptoms resolve completely [1]. Achieving the expected grown-up target stature is attainable if, during treatment with levothyroxine (LT4), skeletal bone maturation is not accelerated too quickly [9]. An ovarian torsion may be a complication occurring in this syndrome. Then, the surgical treatment is used [1].
Here, we discussed a case of a 7-year-old and a 5-month-old female patient who reported severe bleeding from the genital tract. Eventually, the girl was diagnosed with the VWGS. The purpose of presenting this case is to underline the importance of determining TSH levels and thyroid hormone concentrations during the diagnostic process of PP.
Case report
A female patient at 7 years and 5 months old presented to the Admission Room of Gynecological Obstetric Clinical Hospital of Poznan University of Medical Sciences due to a 6-day history of bleeding from the genital tract. The pelvic ultrasound imaging showed a pubertal uterus with a 6 mm endometrium, an enlarged right ovary with a cyst, and multiple follicles. The left ovary was of standard size. The lab tests showed elevated TSH levels (> 500 μIU/ml), decreased levels of free thyroxine (fT4), and elevated levels of FSH and estradiol (E2); LH was undetectable. There was tranexamic acid applied in the Admission Room to stop the bleeding, and the girl was sent to the pediatric endocrinologist.
Patient was admitted to the Department of Pediatric Endocrinology. In addition to the bleeding, the girl had also experienced increased drowsiness and fatigue, had gained 10 kg in 10 months, her skin had become dry, and she had found it more difficult to do sports. She has not suffered from any chronic disease; she had not taken any medications. She was a premature baby born at 34 weeks; her weight was 2,650 g, her length was 47 cm, and she scored 9/10/10 on the Apgar scale. On the first day of life, she underwent surgery for omphalocele. Her family history was positive for thyroid diseases – her mother suffered from Graves’ disease, while her father and grandmother suffered from autoimmune thyroiditis.
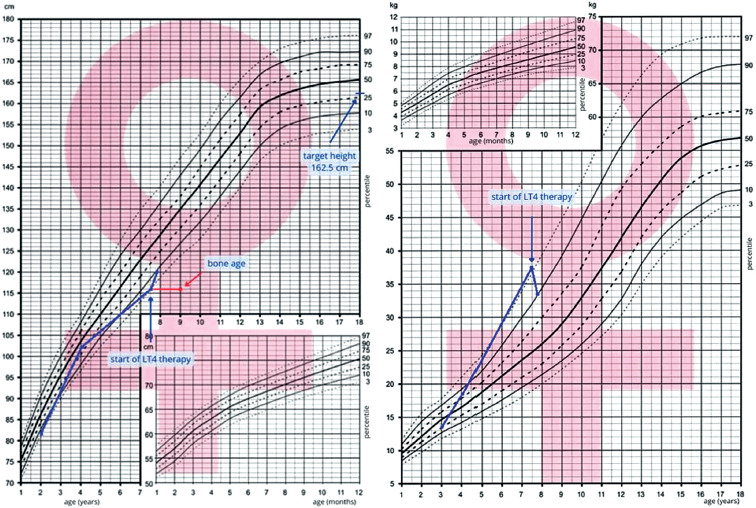
Upon examination, her height was 116 cm (3rd–10th percentile), with an MPH estimated at 162.5 cm (25th–50th percentile). There was a significant decline in height velocity compared with previous measurements (Fig. 1). Her weight was 37.5 kg (> 97th percentile), and her BMI was 27 kg/m2 (> 97th percentile). She was overweight, and her skin was yellowish and waxy (Fig. 2). There was also a scar after her past surgery on her abdomen. Her pulse rate was 70 beats/min, but the cardiac sounds were soft. Her thyroid gland was impalpable. Her sexual development at the Tanner scale was stage 2.

At admission to the Department of Pediatric Endocrinology, the girl underwent laboratory tests (Table I). TSH was above the upper limit of quantification, whereas free thyroxine (fT4) and free triiodothyronine (fT3) were below the reference range. Anti-thyroid peroxidase antibodies (TPO-Abs) and anti-thyroglobulin antibodies (Tg-Abs) were positive. The results of these tests, along with the result of thyroid gland ultrasound (US) imaging (Fig. 3), allowed for the diagnosis of autoimmune thyroiditis (AIT) with primary hypothyroidism.
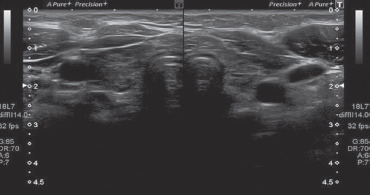
Table I
Laboratory parameters in the presented patient
[i] 25-OH-D3 – 25-hydroxyvitamin D3; APTT – activated partial thromboplastin time; CK – creatine kinase; E2 – estradiol; FSH – follicle-stimulating hormone; fT3 – free triiodothyronine; fT4 – free thyroxine; Gly – glycemia; Hb – hemoglobin; HDL-C – high-density lipoprotein cholesterol;
INR – international normalized ratio; LDL-C – low-density lipoprotein cholesterol; LH – luteinizing hormone; LT4 – levothyroxine; PLT – platelet; PRL – prolactin; RBC – red blood cell; T-C – total cholesterol; TG – triglycerides; Tg-Abs – thyroglobulin antibodies; TPO-Abs – thyroid peroxidase antibodies; TSH – thyroid-stimulating hormone; WBC – white blood cell
In addition, laboratory tests showed that the girl had hyperprolactinemia with concomitant reduced LH level, elevated FSH level, and estradiol (E2) concentration. The patient had hypercholesterolemia with hypertriglyceridemia, normocytic anemia, elevated creatine kinase (CK) level, and elongated activated partial thromboplastin time (APTT). The girl also underwent echocardiography, revealing a trace of fluid in the pericardial sac. The patient’s bone age (X-ray of a wrist) was assessed as nine years using Greulich and Pyle’s radiographic atlas [10]. The abdominal US showed a multicystic lesion in the right ovary (5.1 × 4.4 cm). The patient was diagnosed with GnRH-independent precocious puberty (Van Wyk-Grumbach syndrome). In the girl, LT4 therapy was introduced. The treatment with tranexamic acid was continued until the bleeding stopped. Vitamin D3 supplementation was also applied. After two days of hospitalization, the bleeding had already disappeared. The patient was discharged home in the same condition.
After four months of treatment, it turned out that the girl’s weight decreased by four kilograms in comparison to her weight, as stated at her first hospitalization in the Department of Pediatric Endocrinology. In addition, her TSH level was 5.040 μIU/ml, value only slightly above the reference range. It revealed the correct concentrations of fT3, fT4, prolactin (PRL), and CK. TPO-Abs and Tg-Abs were still detected. Prolonged APTT and hypertriglyceridemia were also observed. In the US examination of the abdominal cavity, the right ovary was not visible, the left ovary was partially visible, and its structure was solid with small follicles.
At the last follow-up, almost eight months into the therapy, the TSH level was slightly elevated (5.30 μIU/ml), with fT3 and fT4 concentrations within the normal limits. The patient also still had hypertriglyceridemia and prolonged APTT. The ultrasound imaging revealed at that time that the condition of the genitals was normal, and there were no focal lesions in the right ovary. Another positive aspect of our patient was the intended weight loss to optimize the body mass index.
Discussion
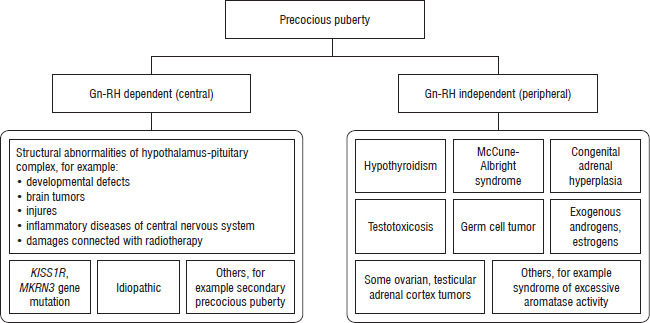
Two PP types are recognized – central PP (CPP), also named GnRH-dependent PP, and peripheral PP (PPP), GnRH-independent PP. Unlike CPP, PPP is not associated with the central activation of the hypothalamic-pituitary-gonadal (HPG) axis and typically arises from genetic or acquired disorders [11–14]. Here, we highlighted the elevated TSH and profound primary hypothyroidism as causes of PPP symptoms (Fig. 4).
In this case, the primary symptom prompting evaluation was genital tract bleeding, which is not typically associated with hypothyroidism. In addition, her sexual development was at Tanner stage 2, with dominating adipose tissue on palpation, which did not arouse suspicion of the CPP. However, further examination revealed additional findings, including increased sleepiness, weakness, weight gain over 10 months, reduced exercise tolerance, dry skin, and decreased height velocity, suggesting thyroid gland dysfunction. Notably, a positive family history of autoimmune thyroid diseases on both the maternal and paternal sides further heightened this concern. While delayed puberty is a hallmark of hypothyroidism in prepubertal children, severe and prolonged hypothyroidism can paradoxically lead to premature puberty, raising the possibility of VWGS. No acceleration of growth rate was observed in the presented girl, which is often a characteristic symptom in patients with PP, but a loss of growth rate due to hypothyroidism. On the other hand, accelerated skeletal maturation by almost 2 years has been documented, which is atypical for VWGS but characteristic of other forms of PP. This unusual finding in our patient was most likely related to prolonged exposure to elevated E2 levels, probably obesity-associated hyperinsulinemia, or a combination of these factors. It is plausible that the coexistence of obesity-related metabolic alterations (an overweight tendency was observed from early childhood) and sustained estrogen stimulation acted synergistically to advance bone age.
In the presented case, laboratory data showed severe hypothyroidism coexisting with elevated E2 and PRL and suppressed LH concentrations. The discordance between FSH and LH results from high PRL due to increased TRH production in primary hypothyroidism. Excessively high TSH levels directly stimulate FSH receptors in the gonads via “specificity spillover”, resulting in increased E2 production, which facilitates the development of secondary sexual characteristics. It promotes follicular maturation and multicystic ovarian changes, particularly during the peripubertal period, consistent with our patient. Multicystic ovaries can range in size from slightly enlarged to massive, potentially mimicking neoplastic lesions and posing a risk of unnecessary ovarian surgery. Prolactin may further exacerbate ovarian sensitization to gonadotropins, accelerating follicular maturation, as seen in this case [1, 4].
Additionally, excessive TRH stimulation may cause feedback adenoma or pituitary hyperplasia, necessitating an magnetic resonance imaging evaluation of the pituitary gland [1, 4]. In a patient with PP symptoms and ovarian cysts, in differentiating diagnostics, McCune-Albright syndrome (MAS) should be taken into consideration. The presence of other typical features of MAS helps clinicians to establish the proper diagnosis [15].
Normal prepubertal ovaries contain numerous follicles up to 9 mm in diameter. By contrast, ovarian cysts in this period are defined as lesions exceeding 20 mm. While these cysts are often benign and asymptomatic, some may be hormonally active, leading to the development of secondary sexual characteristics. Persistent ovarian cysts, however, raise the suspicion of a neoplastic process. Ultrasonographic imaging can help differentiate common functional ovarian changes, such as hemorrhagic and straightforward cysts, from rarer conditions, like chocolate cysts or benign and malignant neoplastic lesions. MRI and tumor marker assays are essential for assessing the nature of an organic cyst before surgical intervention [16, 17].
In this case, replacement therapy with LT4, followed by correction of clinical and laboratory hypothyroidism, led to regression of precocious pubertal signs and improved growth outcomes.








