
Introduction
Chronic liver disease (CLD) affects over 1.5 billion people worldwide [1], and the prevalence of CLD is rapidly rising, in particular due the increasing number of individuals with nonalcoholic fatty liver disease (NAFLD). CLD can have different aetiologies, including viral hepatitis, autoimmune liver diseases (autoimmune hepatitis (AIH), primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC)), alcoholic liver disease (ALD), and metabolic and genetic conditions (Wilson’s disease, haemochromatosis) [1, 2].
The management of CLD is commonly focused on the prevention of progression to cirrhosis through the effective treatment of the underlying liver disease, the treatment of the complications of cirrhosis in the setting of end-stage liver disease and, where necessary, liver transplantation. The management of symptoms has previously been of secondary importance [3]. Now, however, it is being increasingly recognised that CLD can impair quality of life (QoL). Related changes include increased fatigue, non-encephalopathic cognitive impairment, autonomic dysfunction, a loss of appetite, or mood alternation (anxiety, depression) [4, 5]. These symptoms can occur at any stage of liver disease and may not be alleviated with treatment of the underlying process. The most common symptom reported by patients with CLD is fatigue [4–6]. Fatigue is common and is experienced by everyone during their lives, but it is a complex symptom that includes lethargy, exhaustion, and malaise. It can present as a specific clinical problem or as an occult problem not linked to liver disease; this makes it easy to miss in clinical assessment. The management of extrahepatic symptoms and their impact on QOL is an important aspect of treatment for CLD patients.
The aim of this review is to highlight the problem of fatigue in CLD, the current theories on its pathogenesis, and, perhaps most importantly to patients, current treatment approaches.
Prevalence of fatigue in CLD patients
The term “fatigue” can be used to describe a subjective sense of weakness in terms of difficulty initiating any activity, readily becoming tired during activities, or a mental tiredness involving difficulties with concentration, memory, and emotional stability [7]. Careful history examination has revealed that patients often describe fatigue as sleepiness or an uncontrollable need to sleep. Acute fatigue is defined as fatigue lasting for one month or less, subacute fatigue as lasting between 1 and 6 months, and chronic fatigue as lasting for over 6 months [8].
Most studies on fatigue in CLD patients separate it into 2 types: peripheral and central. Peripheral fatigue is manifested by muscle weakness and is associated with neuromuscular dysfunction at the peripheral nervous system and muscular levels [5, 9]. Recent studies [10] have described muscle metabolism changes in patients with CLD, but, in general, peripheral fatigue is not a major problem in the early stages of CLD. On the other hand, it causes the main burden in the setting of cirrhosis and liver failure, where it is associated with sarcopaenia and increased muscle catabolism [5].
Central fatigue, which results from changes in neurotransmission within the brain, is characterised by a lack of self-motivation to initiate or sustain attentional tasks. Because of its central origin, it can overlap with other neuropsychiatric symptoms such as depression and anxiety [5, 9, 11].
Fatigue is a common complaint among CLD patients, with a prevalence of between 50% and 85% [12] (Table I). It mostly interferes with physical activity, family life, and the ability to work [13]. Fatigue has been best characterised in the context of PBC [14, 15], along with the development of special tools and diagnostic criteria [16, 17], but it is worth mentioning that it may also affect everyday activities in a significant proportion of patients with NAFLD and ALD [18]. Moreover, it may play an important role in the course of drug-induced liver injury (DILI) [19]. Fatigue is a significant problem for patients who have acute presentation of viral and autoimmune hepatitis, and it often corresponds with hepatic inflammation. It usually subsides while antiviral or immunosuppressive treatment is being received [11, 20, 21]. On the other hand, it is well documented that fatigue reduces the QoL in patients with chronic hepatitis C (HCV) because it can impair cognitive abilities and reduce work performance and is associated with a higher prevalence of depression in this group of patients [11, 20]. Inversely, there is less evidence for the impact of fatigue on chronic hepatitis B (HBV) patients who have been shown, in some studies, to have QoL scores similar to those of healthy controls [11, 22]. In summary, the severity of fatigue is not related to the severity of CLD, so CLD management will not necessarily ameliorate fatigue symptoms.
Table I
Prevalence of fatigue in different liver disorders
| Condition | NAFLD | ALD | AIH | PSC | PBC | DILI | HBV | HCV |
|---|---|---|---|---|---|---|---|---|
| Prevalence of fatigue | 70% [18] | 75% [18] | 50% [55] | 35–50% [56] | 68–85% [39] 45% [15] | 40% [19] | 90% [57] | 50% [58] |
Chronically fatigued CLD patients should be under special supervision, which is almost impossible to achieve in the real world, but fatigue may negatively impact patients’ survival. Follow-up studies conducted in a geographically defined cohort of PBC patients showed that higher fatigue scores at baseline are associated with significantly reduced survival rates [23]. The mechanism associated with this relationship is yet to be determined.
Pathophysiology of fatigue in CLD
The pathogenesis of fatigue in CLD remains unclear. The most popular concept assumes the existence of peripheral pathways between the liver and brain which, when activated, can lead to neurotransmission changes within the brain and the development of sickness-associated behaviours, including fatigue (Figure 1) [6, 24].
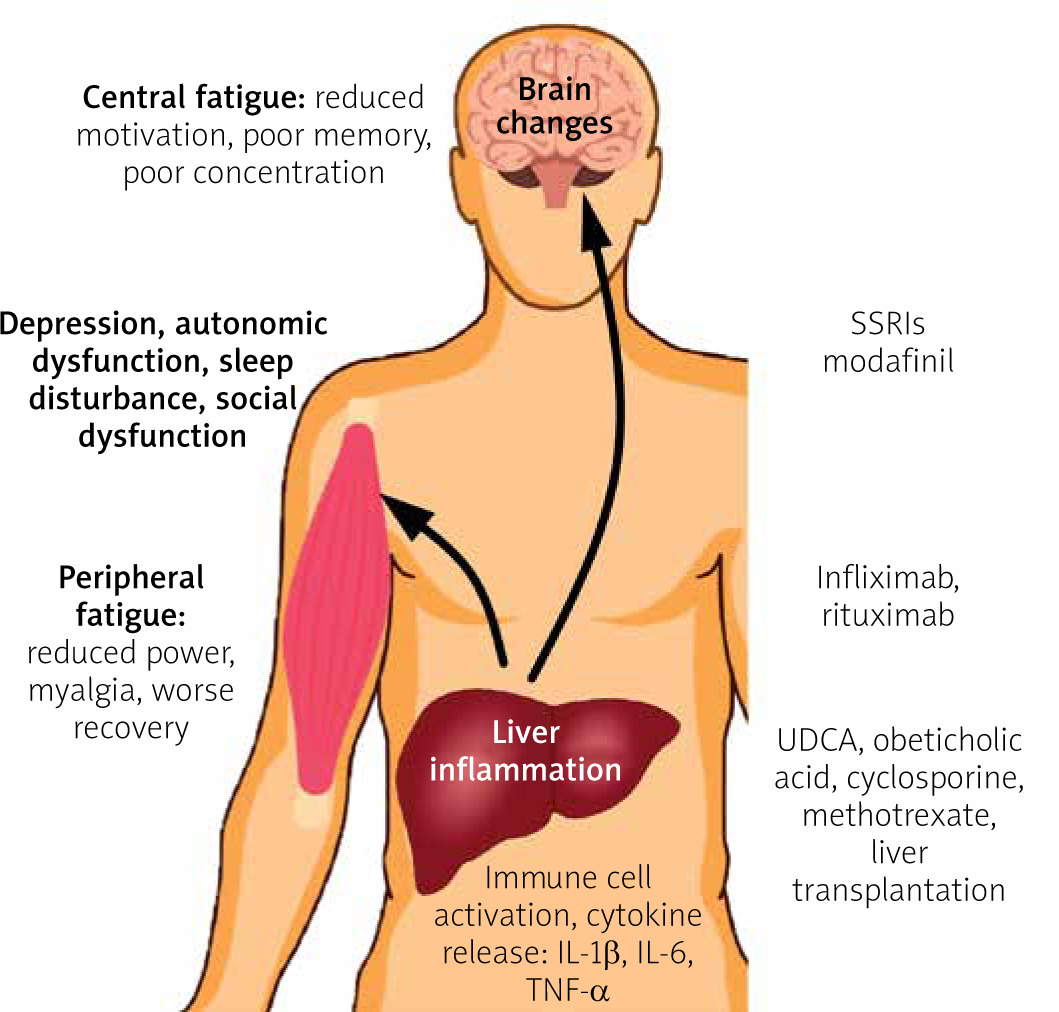
The inflammation of the liver involves the production of increased amounts of inflammatory cytokines, such as interleukin (IL) 1β (IL-1β), IL-6, and tumor necrosis factor α (TNF-α), which can affect brain neurotransmission via neural routes through the activation of vagal nerve afferents, or via a humoral route when carried to the brain within the blood circulation. Both of these routes can directly or indirectly modify brain neurotransmission through the stimulation of cerebral endothelial cells and microglia. On the other hand, liver inflammation is associated with the activation of immune cells that are carried within the circulation and can enter brain parenchyma. Activated immune cells can initiate inflammation within the brain through local cytokine release, which leads to neurotransmission changes. The pathogenesis of central fatigue is linked to alterations in neural pathways associated with the regulation of motivational and reward behaviours. The occurrence of CLD can contribute to changes in the basal ganglia [6, 11].
One of the potential factors modulating the brain–liver axis is the gut microbiome. Recent data suggest that it plays roles in mood disturbances and behavioural changes in the setting of CLD [25]. A study conducted in an animal model of cholestatic liver disease showed a reduction in sickness-associated behaviours after administration of the probiotic mixture VSL#3 [26]. Because of the increased gut permeability and interruption of the detoxication process, increased levels of endotoxin are found in patients with CLD. Endotoxin is a TLR4 ligand, and TLR4 was recently identified as a key regulator in signalling between activated immune cells and the brain [27, 28]. This suggests that manipulation of the gut microbiome using pro- or pre-biotics may be a promising option for the treatment of extrahepatic symptoms, including fatigue, in CLD patients.
Studies on inflammatory diseases, such as rheumatoid arthritis (RA) and inflammatory bowel disease (IBD), have confirmed a link between elevated levels of the circulating proinflammatory cytokine TNF-α and the development of fatigue [29]. In the setting of CLD, similar data have emerged from animal model studies [4]. A study of over 2000 PBC patients confirmed the presence of an association between fatigue and autonomic vasomotor dysfunction, which leads to postural hypotension and secondary tachycardia [15]. Interestingly, in the DIANA study, elevated TNF-α levels were linked to autonomic dysfunction in arthritis patients [30]. This suggests that the inhibition of TNF-α production may be the next approach for treating fatigue and associated autonomic dysfunction in CLD patients.
Advanced imaging techniques allow us to describe changes within the central neural systems of fatigued patients. In a study of PBC patients, changes were described in the basal ganglia [31]. The basal ganglia contain subcortical nuclei, such as the subthalamic nucleus, globus pallidus, substantia nigra, and striatum, which, respectively, contain the nucleus accumbens, putamen, and caudate nucleus. They regulate the motor functions and play an important role in processes like learning, motivation, and reward-guided behaviour. They are connected to the brain cortex through the striatal–cortical pathway. One hypothesis postulates that changes in the basal ganglia can lead to the development of central fatigue by interrupting the scheme of motivational behaviour and the effort–reward balance [32]. These findings have also been observed in patients with structural changes within the basal ganglia during the course of neurologic diseases such as multiple sclerosis and Parkinson’s disease, who also suffered from fatigue [32, 33]. Structural changes in the basal ganglia can be observed in cirrhotic patients, but in PBC they can occur at the early stages of the disease, even within 6 months of diagnosis [34]. The pathomechanism of these changes is still unclear and needs further investigation.
Normal neural activity results from correct interactions between various neurotransmitter systems. There is no specific pathway that regulates fatigue, but dopaminergic and serotonergic neurotransmission seems to be a key factor. Dopamine is a central neurotransmitter involved in the regulation of reward and motivational behaviour, which is responsible for signalling within the basal ganglia. Any imbalance in the dopaminergic system due to either central (e.g. multiple sclerosis, Parkinson’s disease) or peripheral (RA, liver disease) inflammation leads to decreased motivation and fatigue [35, 36]. On the other hand, mood alternations and anxiety are commonly associated with serotonin. Serotonergic neural pathways can regulate dopamine release in the basal ganglia through stimulation of its receptors, such as 5-HT1A and 5-HT3. In the clinical setting, the administration of the 5-HT3 antagonist ondansetron has been associated with the amelioration of fatigue in HCV patients [37]. Interestingly, there was no improvement in patients with PBC [38]. This can probably be explained by the occurrence of serotonergic neurotransmission alternations in HCV patients. Because of the close relationship between the dopaminergic and serotonergic neural pathways, central fatigue can be complicated by other neuropsychiatric symptoms such as depression and anxiety. In a study of PBC patients, 44.8% met the criteria for the diagnosis of depression based on the Beck Depression Inventory (BDI). This study also identified a significant correlation between the level of fatigue and the presence of depression, which suggests that severe fatigue may induce secondary depression [39]. Moreover, it is difficult to distinguish between fatigue and depression using standard questionnaires. A study on depression in PSC and PBC revealed that 42% of patients had depressive symptoms based on the self-report BDI scale, but when interviewed using a structured psychiatric interview, only 3.7% met the DSM-IV criteria for depressive syndrome [40]. The authors suggested that fatigue in patients with PSC and PBC cannot be explained by depression. This also underlines that most depression questionnaires include questions about fatigue-related symptoms.
Management of fatigue in CLD
Pharmacological treatment
Because of the impact of fatigue on the QoL of patients with PBC, most interventions used to alleviate this symptom have been performed on this specific group of patients. These interventions include 2 types of strategy: PBC-specific therapies and fatigue-directed therapies. The first group includes the use of ursodeoxycholic acid (UDCA), obeticholic acid (OCA), fibrates, and liver transplantation (LT). UDCA is commonly known to be effective for the treatment of PBC, and it reduces the risk of death and liver transplantation. However, a recent meta-analysis showed no improvement regarding the relative risk of fatigue after treatment with UDCA [41]. Similarly, the only study on fatigue outcomes after the use of OCA demonstrated no improvement [41]. Based on a recent meta-analysis, LT reduced fatigue in PBC patients, but PBC patients with fatigue remain more fatigued after LT than controls [42]. These arguments confirm that effective treatment of the underlying liver disease does not reduce fatigue nor indicate the extrahepatic cause of fatigue. Fatigue-directed therapies involving the use of the selective serotonin reuptake inhibitors (SSRIs). Fluvoxamine [43] and fluoxetine [44] have also been shown to be ineffective in patients with PBC with no concomitant depression. There are no data on the effectiveness of this type of therapy for treating fatigue in patients with co-existing depression. Initial studies on modafinil, an eugeroic, showed a reduction in daytime sleepiness and a decrease in fatigue scores, bringing some promising data into the field [45, 46]. However, a long-term study and randomised controlled trial did not demonstrate the efficacy of modafinil in the treatment of fatigue in PBC patients [47].
Observations from immune-mediated inflammatory diseases (RA, IBD) indicate that the use of anti-TNF-α agents is associated with a significant reduction in fatigue [48]. Anti-TNF-α agents are effectively used for the treatment of refractory autoimmune hepatitis [49]. Despite the high cost and risk of severe side effects, this kind of therapy could be considered for the treatment of severe fatigue in CLD patients in the future. On the other hand, the inhibition of TNF-α production is one of the mechanisms of action of other promising agents, like pentoxifylline (PTX) and S-adenosylmethionine (SAMe). PTX has been shown to reduce fatigue and the clinical course of NASH [50]. Therefore, it may be considered in future studies on CLD. Supplementation with SAMe, the most important methyl donor in humans, was observed to have beneficial effects on liver biochemistry and extrahepatic symptoms, including reduced fatigue in patients with cholestatic liver disease [51, 52]. However, although this agent is in use in many centres worldwide, there are still a lack of solid data to implement this treatment in everyday practice.
Nonpharmacological strategies
As specific pharmacological interventions for fatigue in CLD patients are limited, supportive management is currently recommended. An example of a structured approach that was initially developed for the management of fatigue in PBC is TrACE (Treat, Ameliorate, Cope, Empathise) (Table II) [53]. It can be applied to all extrahepatic symptoms in all CLD patient groups. Direct management should be focussed specifically on identifying and treating the underlying liver disease and non-disease-specific causes of fatigue (e.g. hypothyroidism in PBC or type 2 diabetes in NAFLD) (Table III). This intervention represents the “treat” element of the approach. The “ameliorate” element of the algorithm involves the identification and modification of factors that can worsen fatigue, e.g. sleep disturbances, autonomic dysfunction, itching, etc. At this point, there are some specific interventions that can be used, such as advising the patient about sleep hygiene, increasing fluid intake, or taking care when standing from a lying position in patients with autonomic dysfunction. It is worth mentioning modafinil because it can be useful to treat daytime somnolence in PBC patients. Moreover, where possible, it is suggested that drugs that can exacerbate fatigue are discontinued (e.g. β-blockers). It is crucial for patients to retain ownership of the problem and for clinicians to be there to help to create strategies to “cope” together. This element consists of lifestyle changes, which should be openly discussed with patients. These changes may include a reduction in workload, a gradual increase in physical activity, or the provision of individual or group therapy. Cognitive behavioural therapy may play a beneficial role in managing fatigue for some patients [54]. The final point of this concept is to “empathise”. Clinicians need to be understanding and aware of their abilities and barriers in the management of fatigue in CLD patients.
Table II
The TrACE approach to the management of fatigue in CLD patients
Table III
Differential diagnoses of causes of subacute and chronic fatigue
Conclusions
Fatigue continues to represent a major, but commonly unrecognised, debilitating symptom in patients with chronic liver diseases. Therefore, there is a need to increase the awareness of the impact of extrahepatic symptoms during the course of CLD. Much effort has been expended to explain the potential drivers of fatigue in CLD, but our knowledge in this area remains incomplete. A better understanding of the underlying pathophysiological mechanisms may provide new therapeutic options, which will bring relief from this debilitating symptom. Despite the lack of targeted therapies, fatigue should be managed through a supportive approach.











