
INTRODUCTION
Acrodermatitis chronica atrophicans (ACA) is a late chronic subtype of Lyme disease which occurs after years of untreated disease [1]. Lichen sclerosus (LS) is a chronic inflammatory disease of uncertain pathogenesis, which may affect people of different ages [2]. In some cases, it is possible for both entities to overlap.
OBJECTIVE
Presentation of an unusual case of ACA and LS coexistence with a brief review of the literature.
CASE REPORT
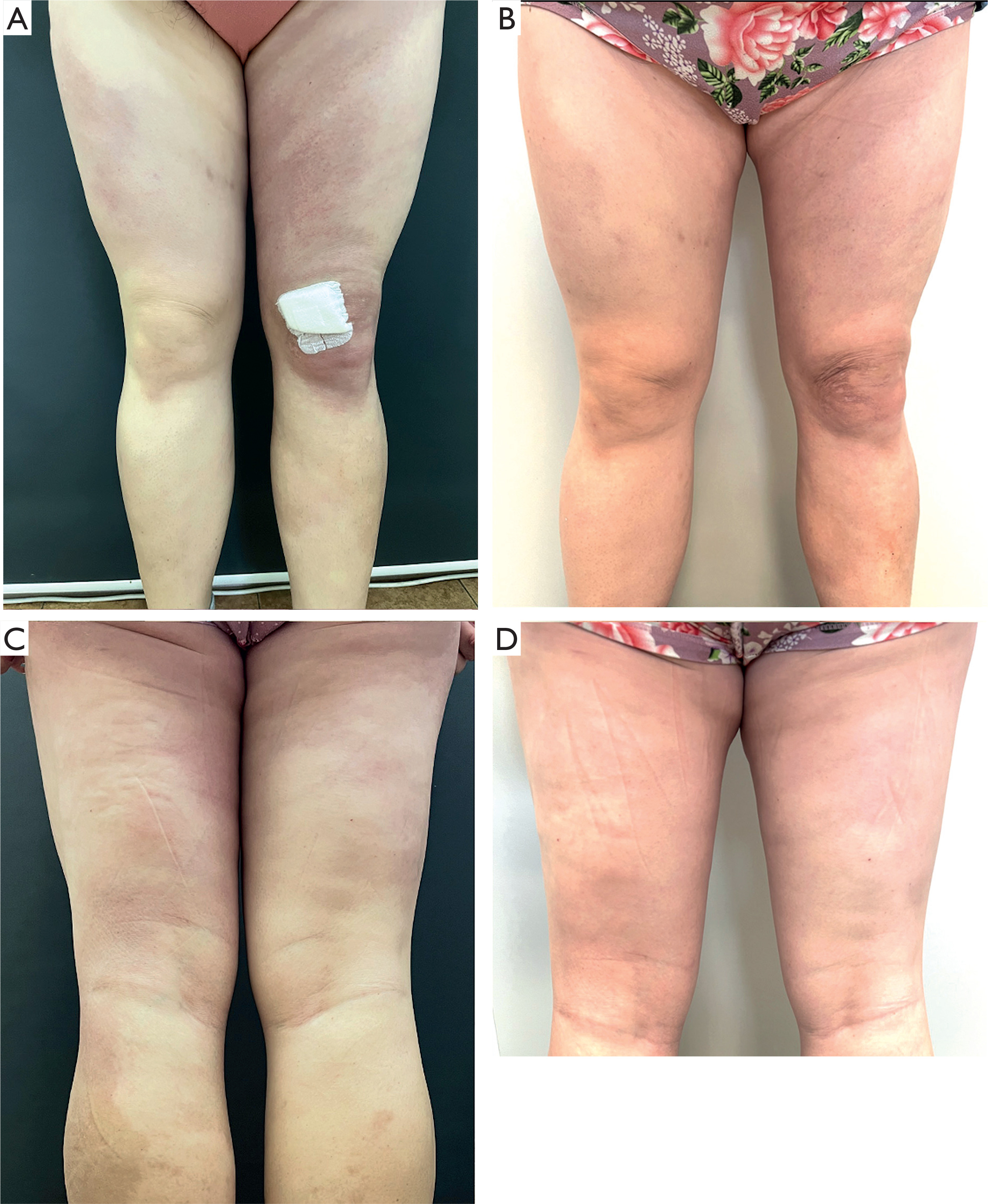
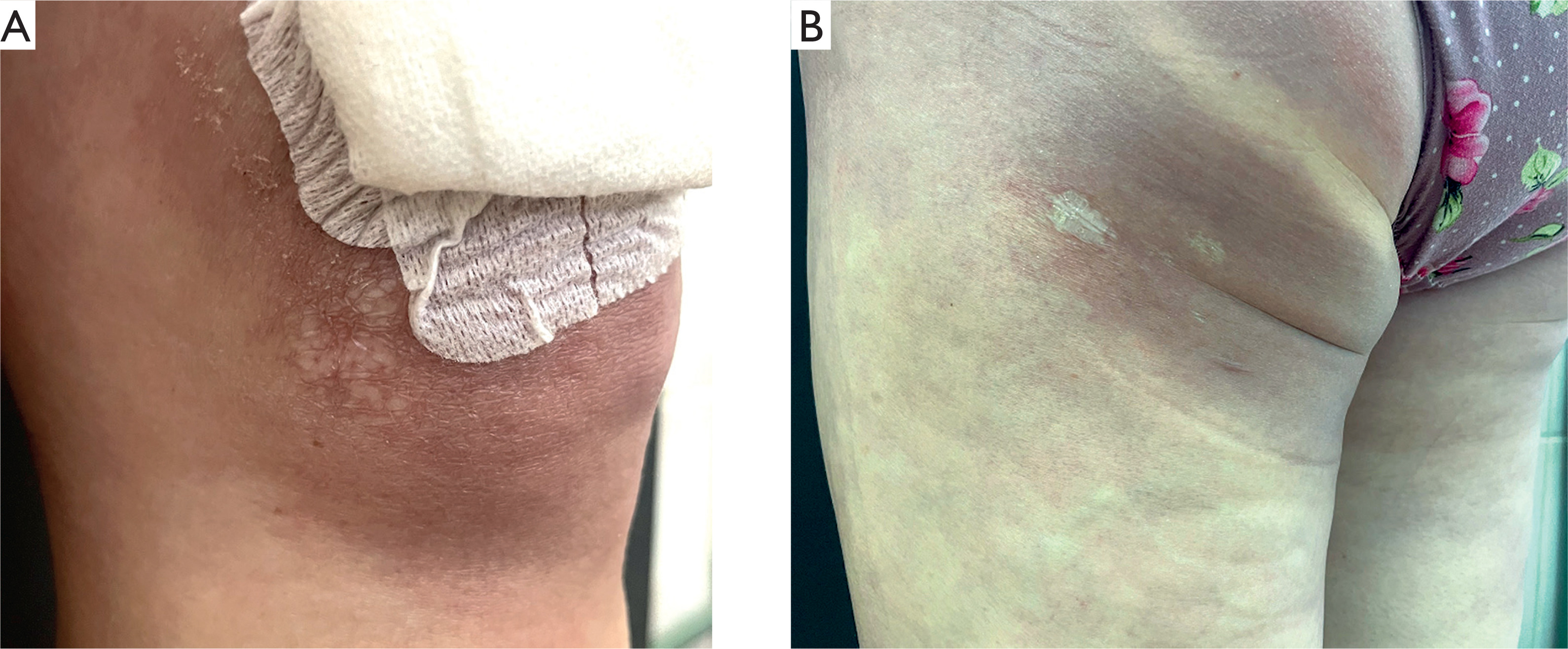
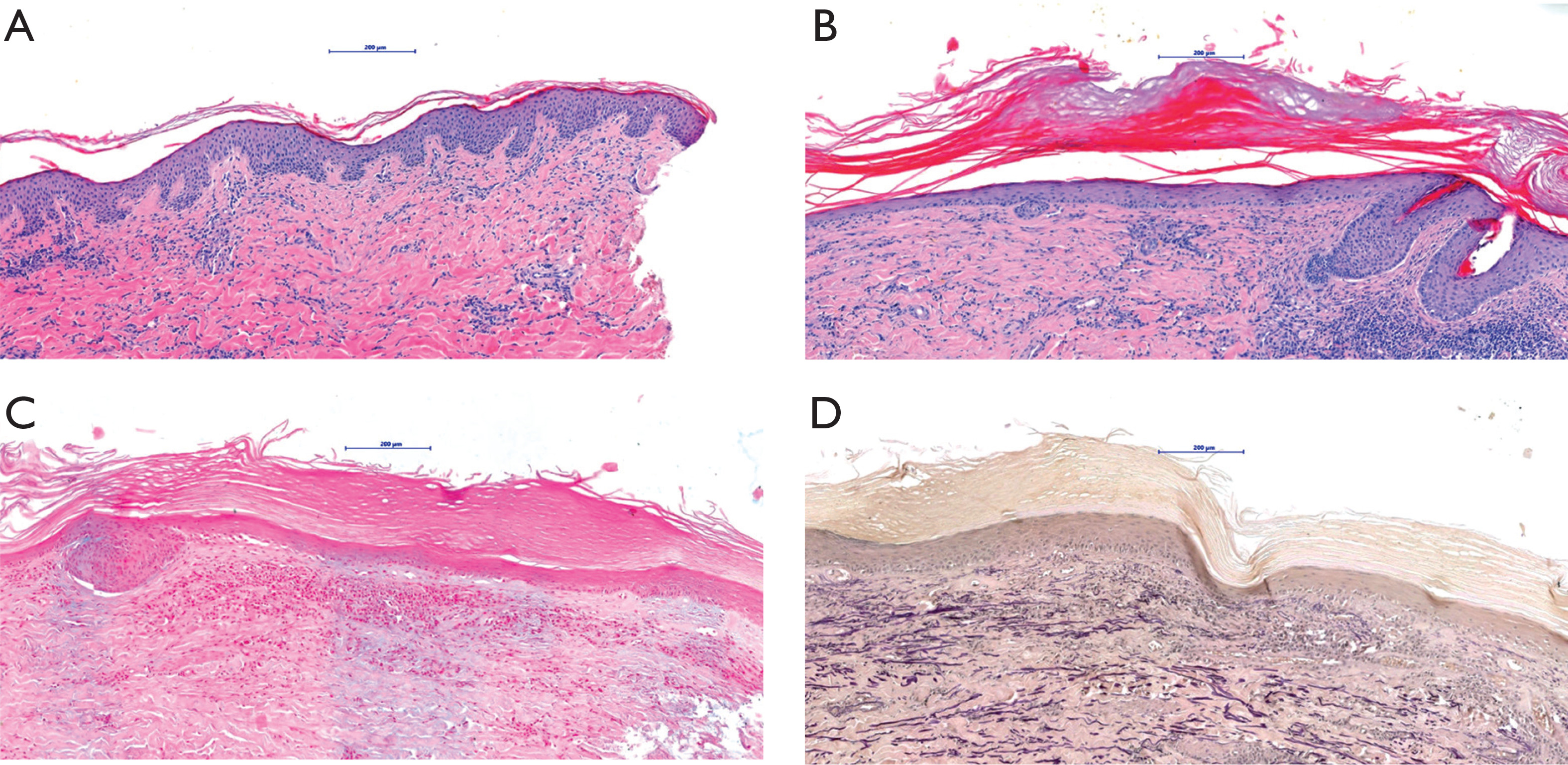
A 38-year-old woman was admitted to the Department of Dermatology due to extensive macules located on the lower limbs persisting for 2 years. She did not notice any association between skin lesions and any potential triggering factors, including tick bites; however, she lived in an endemic area for tick-borne diseases. On the physical examination, there were purple-pinkish macules observed on the thighs and buttocks, which were very firm on palpation (Figures 1 A, C). Moreover, there were several white-silverish papules on the knees and a patch on the buttock present (Figures 2 A, B). There were no abnormalities in the basic laboratory investigations. The IgM and IgG antibodies against Borrelia were both positive in ELISA, confirmed in western blot examination. One skin biopsy was taken from the hardened lesions on the buttock and it revealed lymphohistiocytic infiltration, few plasma cells, and fibrosis in the dermis (Figures 3 A, B), which altogether, along with the clinical and laboratory findings, could be suggestive of ACA. The second biopsy was taken from the white-silverish papules and revealed epidermal thinning and vacuolar degeneration in the basal layer, along with subepidermal lymphocytic infiltration with plasma cells, and moderate fibrosis in the dermis. Orcein staining revealed fragmentation of elastic fibers. There was no increased mucin deposition in alcian blue staining (Figures 3 B–D). LS diagnosis was made. The patient was consulted by the infectious diseases specialist, who introduced doxycycline 2 × 100 mg for 3 weeks. Moreover, she received topical clobetasol ointment alternating with tacrolimus ointment. After 6 months, there was a great improvement in skin condition, the hardening of the skin resolved completely and only pale erythema was observed (Figures 1 B, D), as well as LS papules were flattened.
Figure 1
A, C – before the treatment: purple-pinkish macules observed on the thighs and buttocks, very firm on palpation, B, D – after doxycycline treatment: hardening of the skin resolved leaving visible palor erythema
DISCUSSION
ACA, a late variant of Lyme disease, is usually caused by the infection with B. afzelii and is more frequently observed in Europe [1]. It occurs in two stages: erythematous-oedematous when skin is bluish-purplish and swollen, and second – atrophic – when skin becomes thin and shiny, compared to the ‘cigarette paper’, with visible blood vessels [1]. The main site of skin lesions are the extremities, especially their distal parts [3]. In our patient, the lesions appeared on the lower limbs, including their proximal parts; however, there are reports on ACA lesions located in various body sites, not exclusively distal [4]. The clinical differential diagnosis in the first stage of ACA includes erysipelas and cellulitis, lymphedema, localized scleroderma, cutaneous lupus erythematosus, chronic venous insufficiency or thrombophlebitis, whereas in the second stage, it can also include livedo reticularis or side effects due to the chronic use of potent topical corticosteroids [1]. In the majority of chronic ACA cases, IgG antibodies against Borrelia are positive, whereas IgM antibodies are often falsely positive in late-stage cases and are not useful in diagnosis [1]. Besides serological tests, a biopsy should be performed. The microscopic picture typically reveals a moderate superficial and deep oerivascular, interstitial and periadnexal lymphocytic and plasma cell infiltrate, vacuolar alteration with a subepidermal band-like infiltrate. Later stages exhibit thinning of the epidermis with loss of rete ridges, compact orthokeratosis, thick collagen bundles, and dilated vessels in the dermis [5]. Therapy may consist of doxycycline, amoxicillin, ceftriaxone or cefixime [1].
As for LS, however uncertain, there is some evidence of Borrelia infection being a potential triggering factor of LS [2, 3]. LS manifests as whitish-silverish papules or patches in the genital or extragenital area, whereas the latter is more rarely observed (15–20% of all LS cases) [2]. It is diagnosed based on the clinical presentation or skin biopsy in doubtful cases [2]. The microscopic picture in LS cases differs between early and long-existing lesions but usually features a band-like infiltration of lymphocytes beneath an area of dermal edema underling epidermis with orthokeratotic hyperkeratosis with follicular plugging. In early lesions, there is thinning of the epidermis, vacuolar degeneration of the basal layer of the epidermis, hyalinization of the subepidermal collagen, a reduction in elastic fibers in the upper dermis, and dilated blood vessels beneath the basement membrane. In the late-stage lesions, the number of mononuclear cells decreases within the hyalinized dermis [6]. Treatment encompasses topical steroids, calcineurin inhibitors, phototherapy, or methotrexate [2].
In the available literature, we found only a few cases of ACA and LS coexistence [7, 8]. In the other cases, LS occurred at different body sites, both in the genital and extragenital region [7, 8]. Both dermatoses resolved after antibiotic therapy; however, LS lesions tended to resolve more slowly [7].










