








Introduction
Ankylosing spondylitis (AS) primarily targets the spine and sacroiliac joints, manifesting as a chronic inflammatory autoimmune condition. The condition is marked by the formation of new bone in the axial skeleton and progressive structural deterioration in the spine, sacroiliac joint, and, potentially, peripheral joints. Additionally, extra-articular manifestations such as uveitis, psoriasis, inflammatory bowel disease, and cardiovascular and pulmonary abnormalities may manifest in individuals with this condition [1]. AS predominantly affects young males and is characterized by joint pain and stiffness (ankylosis), accompanied by inflammation at tendon insertions [2,3].
The treatment focus is not only on affecting the inflammatory process but also on preventing structural damage and preserving function. The standard treatment, apart from rehabilitation, consists of the administration of non-steroidal anti-inflammatory drugs (NSAIDs) and disease-modifying antirheumatic drugs (DMARDs). Despite treatment with NSAIDs, treatment with tumor necrosis factor α (TNFis) inhibitors (biological treatment) is recommended in patients with high disease activity [4]. Factors indicating a positive response to TNFis include shorter disease duration, patients aged ≤40 years, lack of enthesitis, HLA – B27 positivity, good functional status, elevated CRP levels [5], and male gender [6]. Contraindications to TNFis include active infection, tuberculosis, advanced heart failure, lupus, multiple sclerosis, and cancer. Biologic medications may be ineffective in AS patients with concurrent vertebral fractures or degenerative intervertebral disc disease [1].
Siman et al. [7] propose a four-phase sequenced rehabilitation protocol for patients with AS. Phase 1 is based on pain relief and improve mobility, phase 2 aims to restore flexibility and postural re-training, phase 3 focuses on aerobic conditioning and strengthening, and phase 4 on activities of daily living and maintenance of function.
Pain is a prominent symptom suffered by AS patients. Liang et al. [8] reported in their study that water therapy has been shown to decrease disease activity and alleviate pain in these patients. However, it does not appear to improve functional capacity or spinal mobility.
Spinal mobility can be improved by physical exercise. However, if spinal mobility exercises, including stretching and strengthening exercises, are combined with soft-tissue mobilization, this translates into significant improvements at the mobility, functional level, lumbar lateral flexion, disease activity, reduction of disability and increasing the quality of life [9]. Equally important is the performance of balance and stability exercises, which, when combined with spa, can increase the duration of maintaining balance and enhance the benefits of physiotherapy [10].
Aim of the work
The aim of this study was to investigate the benefits of biological treatment on the final effect of rehabilitation in patients with ankylosing spondylitis.
Material and methods
Participants
A total of 60 patients (54 males and 6 females) diagnosed with stage II-III AS participated in the study. The mean age of the patients was 45 years, the youngest was 25, and the oldest was 68. All patients were instructed in the conduct of the study and consented to the use of the data obtained for research purposes. 30 patients received treatment at the rheumatology outpatient clinic of a hospital and 30 patients at the highly specialized rheumatology unit focused on biological treatment of resistant inflammatory rheumatic diseases.
Therapeutic intervention
Conventional treatment consists of using NSAIDs, DMARDs (methotrexate), and corticosteroids. Dosing and duration of treatment are determined by the attending physician based on individual patient’s needs.
Biological treatment was individually indicated (dozing and length) according to the disease, patient reaction on treatment, and to the used biological medicines type, and the treatment lasted for a long time. The administration frequency ranged from once per week to once per month, depending on the active substance used. Adalimumab and Etanercept were mostly administered.
The patients underwent physiotherapy 2-3 times per week, supervised by a physiotherapist for 3 weeks. Conventional methods such as kinesiotherapy and manual techniques were applied within physiotherapy, targeting the maintenance or improvement of spine and peripheral joint mobility, releasing shortened muscles, strengthening flaccid muscles, aiming at muscle balance recovery, and, last but not least, maintaining respiratory performance. Due to analgetic and myorelaxing effects, physical therapy, especially electrotherapy and mechanotherapy, was also applied. All of the physiotherapy and physical therapy procedures were applied according to patient’s individual needs and the attending physician’s indications. The patients exercised twice daily an home during the research, which lasted 5-6 months.
Measured variables
From the total number of patients (n=60), 2 groups were formed. The first group (n=30) consisted of patients who received conventional treatment. The second group (n=30) consisted of patients who received biological therapy.
The degree of functional disability and disease activity were assessed in the patients. Functional disability was assessed using the Bath Ankylosing Spondylitis Functional Index (BASFI) questionnaire. The questionnaire consisted of 10 questions, each of which was scored between 0 and 10 points. The resulting scores ranged from 0 to 100, with 0 indicating no disability and 100 indicating maximum functional disability [11,12].
The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) questionnaire was used to assess disease activity. The questionnaire consisted of 6 questions, each of which was scored between 0 and 10 points. The final score ranged from 0 to 60, with 0 and 60 reflecting no and maximal disease activity, respectively [12,13].
Questionnaires were completed at baseline and after completion of 5-6 months of conventional rheumatology/biological treatment. Simultaneously, all patients underwent rehabilitation in an outpatient form, which consisted of kinesiotherapy and physical therapy.
Results
Patients in both groups experienced a significant reduction in functional disability and disease activity (p <0.001) after treatment (conventional/biological and rehabilitation) (Tables 1 and 2).
Table 1
Statistical evaluation of the input and output results of Group 1
| Questionnaire | Input outcome (n=30) | Output outcome (n=30) | p |
|---|---|---|---|
| BASFI | 52±11.17 (76-29) | 35±7.31 (48-22) | <0.001 |
| BASDAI | 22±5.26 (36-15) | 17.5±5.06 (24-6) | <0.001 |
Table 2
Statistical evaluation of the input and output results of Group 2
| Questionnaire | Input outcome (n=30) | Output outcome (n=30) | p |
|---|---|---|---|
| BASFI | 51.5±11.53 (76-29) | 31±4.52 (42-24) | <0.001 |
| BASDAI | 29±8.62 (41-17) | 19±5.23 (28-7) | <0.001 |
Based on the baseline findings, there was no notable disparity in the degree of functional disability between the two patient groups (p>0.05). However, the biological therapy group of patients was found to have significantly higher disease activity (p<0.05), median BASDAI = 29, before the start of treatment, whereas the median BASDAI was equal to 22 in the conventional therapy group of patients (Table 3).
Table 3
Statistical evaluation of the initial results of Groups 1 and 2
| Questionnaire | Group 1 (n=30) | Group 2 (n=0) | p |
|---|---|---|---|
| BASFI | 52±11.17 (76-29) | 51.5±11.53 (76-29) | 0.450 |
| BASDAI | 22±5.26 (36-15) | 29±8.62 (41-17) | 0.012 |
Statistical processing of the outcome results revealed that the biological therapy group of patients had a significantly lower rate of functional disability (BASFI=31) after 5-6 months of treatment compared to the conventional therapy group of patients (BASFI=35) (p=0.032). Disease activity was comparable in the two groups of patients after treatment, with no significant difference (p=0.063) (Table 4), despite the fact that the biological therapy group of patients had a significantly higher rate of disease activity before treatment. In the conventional therapy group of patients, BASDAI improved by an average of 4.5, and in the biological therapy group, by up to 10 points.
Discussion
International guidelines advise that patients with AS should undergo lifelong physiotherapy, as physical activity and movement are crucial for optimizing health throughout the course of the disease [14]. According to the recommendations of Millner et al. [15], complex physical activities can be employed to sustain a favorable clinical status in patients with AS. Dagfinrud et al. [16] also confirmed the benefit of physical therapy including physiotherapy, home exercises, and spa therapy in AS. The same view is presented in the works of Zochling et al. [17] and Wendling et al. [18], who advocate that non-pharmacological treatment of AS should encompass regular exercise, whether through individual or group rehabilitation exercises.
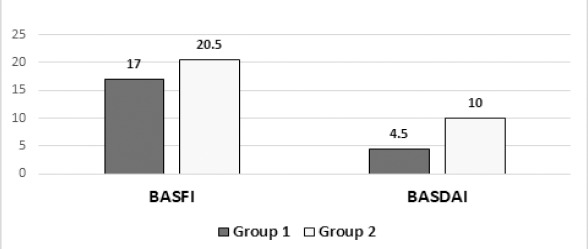
Through our study, we investigated how patients were able to use the potential of rehabilitation to improve their functional status and reduce disease activity after receiving biological treatment. We found that disease activity and functional disability improved in both groups of our patients after receiving appropriate rheumatology and rehabilitation treatment. However, the biological therapy group of patients had a significantly lower rate of functional disability at the outcome examination compared with the group of patients who received conventional rheumatological treatment. However, there was no significant difference in disease activity between the two groups of patients. Nevertheless, if we consider that the biological therapy group of patients had higher disease activity at the initial examination, this means that their BASDAI improved more (by 5.5 points) than that of the conventional therapy group of patients (Figure 1). Physiotherapy has been shown to be essential for increasing functional status in patients with AS [19].
Figure 1
The extent of reduction in functional disability and disease activity
Notes: Group 1 – the group of patients with conventional treatment, Group 2 – the group of patients with biological treatment, BASFI – Bath Ankylosing Spondylitis Functional Index, BASDAI – Bath Ankylosing Spondylitis Disease Activity Index.
Similar results were reached in the study by Levitova et al. [20], when disease activity, assessed by ASDASCRP and BASDAI, exhibited significant improvement in both radiographic and non-radiographic subgroups of AS patients after exercise intervention. Their recommendation is that exercise ought to constitute a vital component of the treatment approach, particularly in the initial phases of the condition. These findings align with research conducted by other authors [21,22] who have also demonstrated the beneficial effect of exercise on reducing disease activity in patients with AS.
Several randomized controlled trials [23-26] have shown that different types of physical activity exert a beneficial influence on diminishing pain and increasing patients’ functional capacity in AS. This result also correlates with the results of our study. Similar results are presented in their reviews by Zochling et al. [27] and Van den Berg [28], where they showed that exercises have a positive effect on functional disability and disease activity, pain and mobility.
Therefore, it is advisable to commence physiotherapy immediately upon the diagnosis of AS, and ongoing regular exercise is fundamental to treatment [29]. Optimal benefit can be achieved with a combination of inpatient spa exercise therapy followed by group physiotherapy, with group physiotherapy being superior and more impactful compared to home exercise. Traditional physiotherapy protocols are advocated, encompassing flexibility, stretching, and breathing exercises, along with pool and/or land exercises.
Based on the results of the study by Tsifetaki [30], individuals diagnosed with AS frequently seek treatment coupled with physical therapy, even when experiencing mild mobility issues. Rehabilitation seems to contribute to enhancing the quality of life for these individuals, though uncertainties persist regarding the required frequency and duration of rehabilitation to sustain its impact.
Our study, despite demonstrating a better effect of physiotherapy in the biological therapy group of patients, has several limitations. One of these is the non-randomized selection of patients. In our region, the population is not high, so the prevalence of spondylarthritis is low. For this reason, we chose the consecutive method of including patients in the study.
The biological therapy group of patients had a significantly lower rate of functional disability in the output results. Considering the information that short disease duration and patient age ≤40 years are predictors of a favorable response to TNFis [5], it follows that these are younger individuals with a shorter disease duration. Therefore, it is less likely that they have degenerative changes in the movement segment that would increase functional disability.
The last limitation is the fact that the biological therapy group of patients had higher disease activity at the initial examination compared to the conventional therapy group of patients. This is because tumor necrosis factor α (TNFis) inhibitors (biological treatment) are recommended solely for patients exhibiting high disease activity [4,5].
Conclusions
The study demonstrated that patients had lower rates of functional disability and disease activity after rheumatic treatment and rehabilitation. Patients who received biological therapy showed better results in the BASFI and BASDAI tests compared to the conventional therapy group of patients, despite having a significantly higher level of disease activity prior to the start of the treatment intervention. Biological treatment has a significant effect on reducing disease activity and allows patients to sufficiently utilize the effect of physiotherapy to increase functional abilities.