
Introduction
Recently, the detection rate of gastric subepithelial tumours originating from the muscularis propria layer (MP-SETs) has increased considerably due to the widespread application of the endoscope and endoscopic ultrasound (EUS) [1]. According to previous studies, a proportion of gastric MP-SETs have malignant potential. Because the pathologic type of these tumours cannot be determined preoperatively, the majority of patients with gastric MP-SETs usually prefer resection over endoscopic surveillance [2, 3].
Currently, 2 main resection methods are used for gastric MP-GISTs, laparoscopic resection (LR) and endoscopic resection (ER), both of which have strengths and weaknesses. LR is usually recommended by surgeons for the resection of gastric MP-GISTs because it has several advantages over open gastrectomy, including fewer complications and shorter hospitalization time [4, 5]. However, LR may result in long-term complications, such as reflux oesophagitis, bile reflux gastritis, or even gastric stump cancer [6]. ER is another alternative for the removal of gastric MP-GISTs. ER can be used to resect gastric MP-GISTs with less damage to surrounding tissues than LR. However, the long-term prognosis of ER for patients with gastric MP-GISTs remains in question. The main point is that the insufficient margins associated with ER might increase the potential risk of residual tumour or recurrence.
At present, there are no selection criteria of ER or LR for the treatment of gastric MP-GISTs between 2.0 cm and 4.0 cm in size [1].
Aim
In this study, we investigated and compared the long-term prognosis between ER and LR for patients with gastric MP-GISTs, with at least 5 years of follow-up.
Material and methods
Study population
We performed this study according to the principles of the Helsinki Declaration II. Moreover, this study was approved by our hospital Ethics Committee. All patients with gastric MP-GISTs, who underwent ER or LR at our institution from January 2010 to December 2015 were consecutively enrolled, and all patients signed informed consent before the ER or LR procedure.
In this study, the inclusion criteria were as follows: (1) the tumours ranged from 2.0 cm to 4.0 cm in size and were diagnosed as a GIST histopathologically after resection; (2) no evidence of lymph node metastasis evaluated by EUS and/or CT preoperatively; (4) patients had not taken anticoagulant drugs for the preceding week and had no blood coagulation disorders before ER or LR; and (5) patients did not have other malignant tumours.
ER procedure
Generally, endoscopic submucosal dissection (ESD) was performed to resect tumors with endoluminal growth, and ESD was performed as previously reported (Figure 1) [7]: (1) Marking dots were made around the tumour, then several millilitres of a mixed solution were injected into the submucosa to produce a submucosal elevation. (2) An electric knife was used to make a circumferential mucosal incision along the marking dots, and then the tumour was excavated by the ESD technique. (3) Finally, an endoscopic lithotripter was used to remove the resected tumour after complete resection.
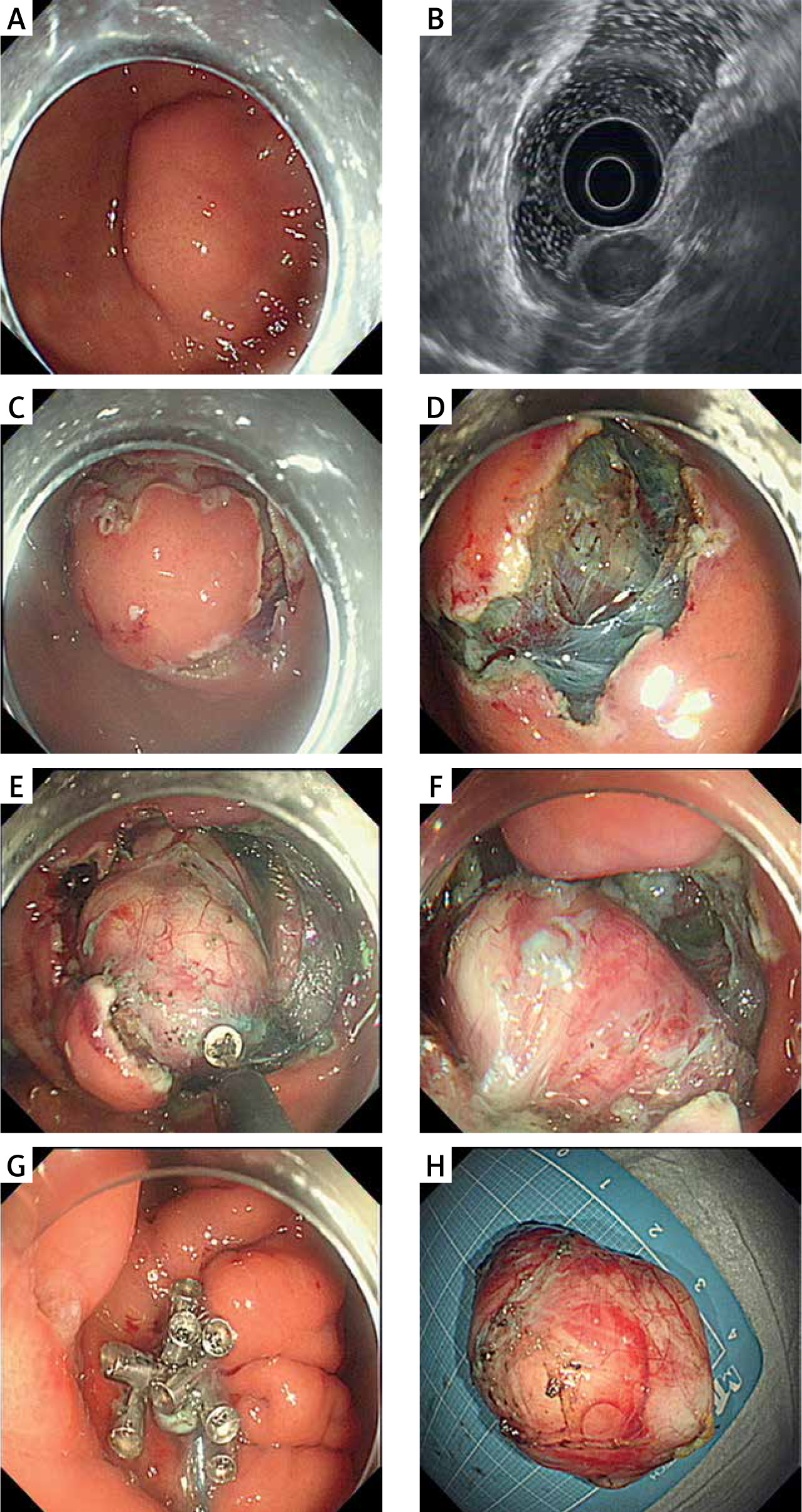
Figure 1
A – Endoscopy showed a subepithelial tumors (SETs) was located in the fundus of the stomach. B – The tumor had extraluminal growth which was evaluated by endoscopic ultrasonography (EUS). C – Circumferential incision was made along several marked dots. D–F – Endoscopic full-thickness resection (EFTR) was performed to resected the tumor. G – Clips combined with an endoloop method was performed for complete closure of the gastric wall defect. H – The resection specimen was a 4.0-cm tumor
When the tumour was tightly adhered to the MP layer or had extraluminal growth, endoscopic full-thickness resection (EFTR) was performed. EFTR was performed as follows [8]: (1) Dots were marked, and a circumferential incision was made, similarly to the ESD method. (2) After the tumour had been fully revealed, an electric knife was used to make a small puncture, along which the tumour was resected. If necessary, a snare was applied for complete resecting of the tumour. (3) An Endoloop combining several clips or an over-the-scope clip (OTSC) was performed for complete closure of the gastric wall defect.
Submucosal tunnelling endoscopic resection (STER) was performed as follows [9]: (1) A 2-cm longitudinal mucosal incision was made as the entrance of the submucosal tunnel, and then a submucosal tunnel was created to reach the tumour. (2) The ESD technique was used to excavate the tumour through the submucosal tunnel. (3) The tumour was removed with a snare or an endoscopic lithotripter after the tumour was completely resected, and then the mucosal incision site was closed with several clips.
LR procedure
Laparoscopic wedge resection (LWR) was as follows [10]: (1) The Veress technique was used to establish a carbon dioxide pneumoperitoneum after making a curved incision below the umbilicus. (2) Four trocars were used (one was inserted in the right costal margin, one in the right anterior axillary line, one in the left costal margin, and one in the left anterior axillary lines). (3) Tumour resection was performed using a laparoscopic linear stapling device. (4) Finally, the resected specimen was put into a bag and extracted through a trocar site. Subtotal gastrectomy was performed when the tumour was located near the cardia or pylorus.
Outcome measures
In this study, the main short-term outcomes included R0 resection, complications related to ER or LR, procedure time, hospital stay, and hospitalization costs. R0 resection was defined as the en bloc resection of the tumour with tumour-free lateral and basal margins [3]. Complications related to ER or LR mainly included perioperative bleeding, delayed bleeding, and localized peritonitis. In the ER group, gas-related adverse events were considered as a complication of ER when the patient required surgical treatment [11].
Long-term outcomes included residual tumour, tumour recurrence, and certain adverse events related to ER or LR. During the first year, endoscopic surveillance was applied at 6 and 12 months to determine whether submucosal protrusion lesions were present within 3 cm of the ER/LR site. If necessary, EUS and deep biopsy were performed to evaluate whether the protrusion lesion was a residual or recurrent tumour. Subsequently, endoscopic surveillance was performed every year.
Statistical analysis
For descriptive statistics, mean ± standard deviation (SD) was used for normally distributed variables, whereas for variables with a skewed distribution, the median was used. Where appropriate, Student’s t test, χ2 test, Fisher’s exact test, or Mann-Whitney U test was used. A p-value < 0.05 was considered statistically significant. Statistical analysis were performed using SPSS 20.0 software (SPSS Inc., Chicago, IL).
Results
Clinical characteristics of the ER group and the LR group
Between January 2010 to December 2015, 134 consecutive patients (ER group, 89 cases; LR group, 45 cases) were enrolled in this study. There were no significant differences between ER and LR with regard to the patients’ clinical characteristics, including age (p = 0.350), sex (p = 0.499), accompanying chronic diseases (p = 0.316), or the distribution of the tumour site (p = 0.250) (Table I). The mean length of the tumour was significantly different between the ER and LR groups (p = 0.001).
Table I
Comparison of clinical characteristics between the endoscopic resection group and the laparoscopic resection group
Comparison of short-term outcomes
In the ER group, 11 tumours were resected by STER, 23 tumours were resected by EFTR, and 55 tumours were resected by ESD. In the LR group, 35 tumours were treated with LWR, and the remaining 10 tumours were treated with subtotal gastrectomy. The distribution of the tumour risk classification was not significantly different between the ER group (low risk, 78 cases; intermediate risk, 9 cases; and high risk, 2 cases) and the LR group (low risk, 38 cases; intermediate risk, 5 cases; and high risk, 2 cases) (p = 0.822).
In this study, the complete resection rate was not significantly different between the groups (97.8% vs. 100%, p = 0.220) (Table II). In terms of complications, 5 (5.6%) patients in the ER group experienced complications, including 2 cases of perioperative bleeding, 2 cases of localized peritonitis, and 1 case of delayed bleeding. In the LR group, 1 patient had anastomotic stenosis after oesophagogastrostomy. No significant difference was observed between the rate of total complications in the 2 groups (p = 0.663). Furthermore, the ER group had a shorter procedure time (50.1 ±18.2 min vs. 120.6 ±32.5 min, p < 0.001), shorter hospital stay (5.1 ±1.9 days vs. 6.4 ±3.7 days, p = 0.026), and lower hospitalization costs (16639.5 ±5091.3 CNY vs. 24030.4 ±6803.1 CNY, p < 0.001) than the LR group.
Table II
Comparison of clinical outcomes between the endoscopic resection group and the laparoscopic resection group
Comparison of long-term outcomes
In this study, 129 patients continued to be observed (ER group, 85 patients; LR group, 44 patients). The other 5 patients were lost to follow-up because of death due to unrelated causes (cerebrovascular disorders, 2 patients; pneumonia, 1 patient; traffic accident, 1 patient). The mean follow-up period was not significantly different between the 2 groups (84.2 ±17.9 vs. 89.0 ±16.8, p = 0.207), and no residual or recurrent tumours were found in either group. In terms of long-term complications, 6 patients had complications in the LR group (reflux oesophagitis, 3 cases; anastomotic ulcer, 2 cases; oesophageal stenosis, 1 case). No patients in the ER group experienced complications during follow-up. Therefore, the long-term complication rates were significantly different between the groups (p = 0.001).
Discussion
In this study, we compared the short- and long-term clinical outcomes between ER (89 cases) and LR (45 cases) for gastric MP-GISTs, with at least 5 years of follow-up. The short-term clinical outcomes showed that the complete resection rates and the total complication rates were not significantly different between the 2 groups, and the long-term outcomes showed that no patients had residual tumours or tumour recurrence during follow-up. These results support the feasibility of both ER and LR for the treatment of patients with gastric MP-GISTs with a tumour size between 2.0 cm and 4.0 cm.
Compared with the LR method, the ER method had the advantage of maintaining the normal anatomy of the stomach when the tumour was located in or near the cardia or pylorus [10–12]. In this study, 12 patients in the LR group underwent cardiogastrectomy or pylorogastrectomy, while all patients in the ER group had normal stomach structure. During the 5-year follow-up, 6 patients in the LR group experienced complications related to the LR procedure, including reflux oesophagitis, anastomotic ulcer, and oesophageal stenosis. In contrast, no patients in the ER group developed complications related to the ER procedure. Therefore, ER may be a preferential procedure for patients with gastric MP-GISTs located near the cardia or pylorus, significantly diminishing long-term complications related to the procedure and enhancing the patients’ quality of life.
Additionally, this study also showed that ER had shorter procedure times, shorter hospital stays, and lower hospitalization costs than LR. These results are consistent with the results of similar studies. Therefore, compared with LR, ER has several advantageous effects including reducing medical costs and saving hygienic resources. From the perspective of health economics, ER is also a preferential procedure for the removal of gastric MP-GISTs [11, 13].
Nevertheless, several concerns have been raised regarding the application of ER for patients with gastric MP-GISTs. Complete resection can be a major concern related to ER for resecting gastric MP-GISTs [14–16]. In this study, however, the complete resection rate in the ER group was not significantly different compared with that in the LR group. For those patients with incompletely resected tumours after ER, further surgical resection was recommended. However, different management approaches should be adopted according to the risk classification. In our institution, for intermediate-risk or high-risk GISTs, further surgical resection and/or imatinib mesylate is generally advised. For low- or very low-risk GISTs, regular endoscopic follow-up is performed [3].
Short-term complications can be another major concern related to ER for the resection of gastric MP-GISTs. Several previous studies have reported that the short-term complication rates related to ER range from 0 to 14.3% [10, 12, 13, 16–18]. In this study, the short-term complications rate was 5.6%, which was within the reported range. Differences of the short-term complications rates in these studies might be due to different definitions of short-term complications and the study inclusion criteria. For instance, in several studies, simple pneumoperitoneum, pneumothorax, or subcutaneous emphysema were not considered as complications because these adverse events did not need special treatment after the application of endoscopic carbon dioxide insufflation. Although the rate of short-term complications in ER was higher than that in LR, it should be noted that most of the short-term complications could be managed effectively by conservative treatments and endoscopic methods, and rarely required surgical intervention. Moreover, these short-term complications usually did not diminish the patients’ long-term quality of life.
There are several limitations to this study. Firstly, selection bias might have been introduced in this study because the tumour size differed between the 2 groups. Therefore, we assumed that the ER group introduced a degree of selectivity in this study. This study was also a retrospective study, and it was only performed in a single hospital, which may have also introduced selection bias. Secondly, our institution is a tertiary endoscopy centre in Eastern China. Therefore, the results in this study may not be generalizable to other institutions. Other limitations include the relatively small sample size and a lack of randomized controls.
Conclusions
ER may be a more feasible and safer alternative to LR for tumours located in or near the cardia or pylorus. This is because ER maintained the normal anatomy of the cardia or pylorus and reduced long-term complications related to the procedure, ultimately enhancing the quality of life of patients in our study. Moreover, ER has several other advantages over LR such as a shorter procedure time, shorter hospital stays, and lower hospitalization costs.










