
Introduction
Colorectal carcinoma (CRC) is the third most frequently diagnosed cancer in males and the second in females [1]. It is the fourth leading cause of cancer-related deaths worldwide [2–5]. CRC can spread by haematogenous and lymphatic dissemination, as well as by contiguous and transperitoneal routes. The metastases of CRC are usually found in the regional lymph nodes, liver, lungs, and peritoneum. At the time of diagnosis, approximately 20% of patients have distant metastatic disease [6]. Bones are an uncommon site of colorectal metastases (10–24%) [7].
When they do appear, they are usually concomitant with liver or lung metastases. According to the study of Santini et al., among patients with bone metastases, the spine is the most common site involved (65%), followed by the hip/pelvis (34%), long bones (26%), and other sites (17%) [8]. Solitary bone metastasis of CRC without other metastasis sites is extremely rare and can be found in less than 1% of patients with CRC [9].
Aim
In the present study, we report the first case of a solitary tibia metastasis and its pathologic fracture as the first presenting feature of a colorectal adenocarcinoma.
Material and methods
A literature search on PubMed and ResearchGate using the keywords “colorectal cancer”, “solitary metastasis”, and “tibia” was conducted. Only English language and full-text manuscripts were included. Each manuscript was reviewed for cases of CRC solitary skeletal metastases to the tibia. Only manuscripts containing an adequate patient description, CRC, and solitary metastasis to the tibia were included.
An isolated case of a patient presenting with a solitary metastasis to the tibia from a rectal cancer at our institution was identified, and a profound review of the patient´s clinical, radiographic, and surgical notes was conducted.
After completing the literature review, 8 cases with solitary metastasis to the tibia from colorectal cancer were found.
Only 3 case reports were deemed to be adequate for analysis [10–12]. Although, it seems that 5 more cases were reported: one by Decker and Fash [13] in 1950, one by Creedon [14] in 1966, and 3 more by Kanthan et al. [15], we found them to be inadequate for literature review. The first could not be retrieved from PubMed, probably due to the late date of publication. Because the cases described by Kanthan were part of a retrospective cohort study, the cases were not specified regarding clinical, radiographic, or surgical data.
Results
Case report
We report a case of a 78-year-old female patient with medical history of hypertension and benign tumour of the uterus for which she had undergone hysterectomy 12 years earlier. She presented at our emergency department due to an atraumatic pretibial swelling of the left leg that she noticed 1 month earlier. Plain radiography did not detect any pathology, although decreased soft tissue transparency around the proximal tibia was seen (Figure 1). Under local anaesthesia the swelling was incised and a serous-bloody collection evacuated. During the procedure the tibial bone surface was found to be irregular, but no further investigations were made, and the patient was discharged. The wound dressing was changed every 2 days in the outpatient service. Swab culture from the incised place was sterile.
Figure 1
Plain radiography reveals altered bone structure of the proximal tibial diaphysis as well as decreased surrounding soft tissue transparency

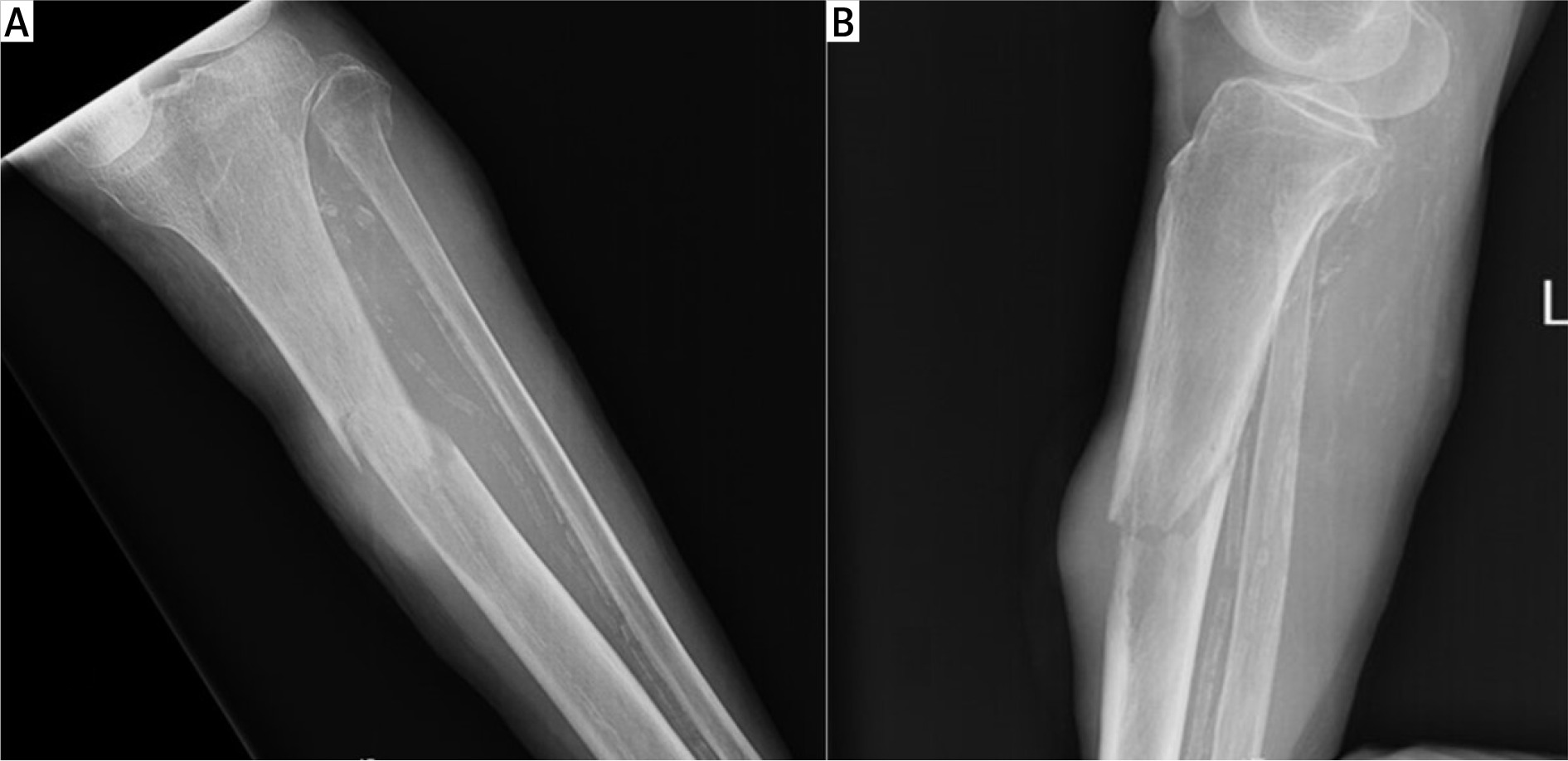
On the 17th postoperative day, during a regular walk, the patient fell and broke a leg. She was brought to our emergency department, where a pathologic fracture of the proximal tibial diaphysis was diagnosed on X-ray, just at the level of the prior incision (Figures 2 A, B). Laboratory analysis showed signs of anaemia with a slightly decreased haemoglobin level (108 g/l; NL 119–157 g/l) and decreased erythrocytes (3.81 × 106/ml; NL 3.86–5.08 × 106/ml). The CA-125 tumour marker was elevated (36.3 kIU/l; NL < 35 kIU/l), and AFP was also slightly increased (11.5 µg/l; NL < 9 µg/l).
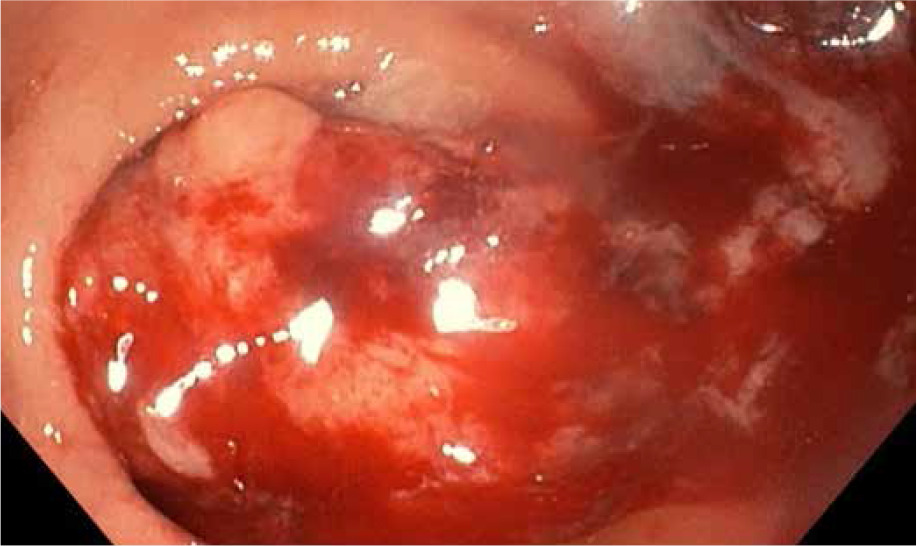
The patient underwent emergency surgery, and osteosynthesis was achieved by means of external bone fixation (Figure 3). Intraoperatively, a biopsy of the altered bone tissue from the fracture site was taken. The pathological examination revealed metastatic colorectal adenocarcinoma. During the hospitalization, a broad diagnostic work-up was undertaken. MSCT of the abdomen, thorax, and lower extremities was obtained and revealed rectal tumour with no signs of metastases apart from the osteolytic lesion in the fractured left tibia (Figures 4 A–C). Furthermore, a colonoscopy was done, and a circular mass in the upper rectum, about 12 cm from the anal verge, was found (Figure 5). Pathological examination of the tumour specimen obtained at colonoscopy confirmed a moderately differentiated primary adenocarcinoma of the rectum. The patient was presented at a multidisciplinary tumour-board, where it was decided to perform a resection of the primary tumour and a femoral amputation prior to chemotherapy.

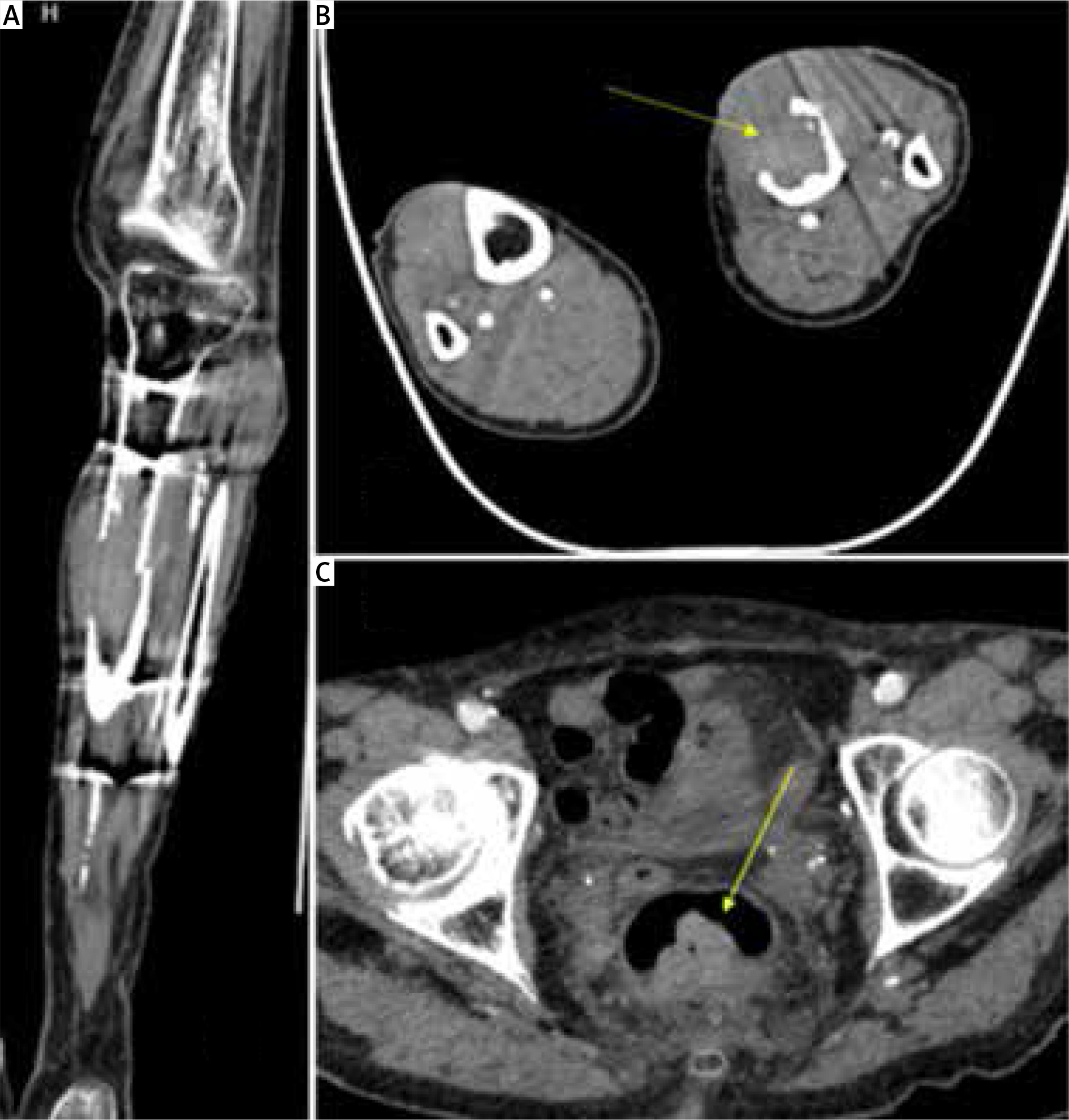
Figure 4
A – Coronal plane of MSCT – osteolytic tibial lesion, B – Axial plane of MSCT – osteolytic lesion in the diaphysis of the left tibia covering almost all the diameter of the bone in this site, C – Axial plane of abdominal MSCT showing rectal mass
Due to the patient’s age and overall status it was decided to perform these 2 operations separately. First, an explorative laparotomy was scheduled, and a tumour of the proximal rectum was found without signs of metastases in the abdomen. An anterior rectal resection was performed. Pathological analysis of the rectal specimen revealed a T3N0 stage, moderately differentiated rectal adenocarcinoma.
The patient recovered well from the operation, and 2 weeks after the anterior rectal resection the femoral amputation of the diseased leg was performed. Pathological examination, including the immunohistochemical profile of the tumour cells of the leg confirmed the diagnosis of metastatic colorectal carcinoma. Microscopically, tumour tissue was composed of atypical adenoid structures with foci of comedo-type necrosis. At the marginal parts of the tumour the bone beds were preserved (Figure 6). Tumour cells showed a positive immunohistochemical reaction to CK8, CK20, BER EP4, and CDX2 (Figures 7–10) and a negative reaction to CK7 (Figure 11, Table I).
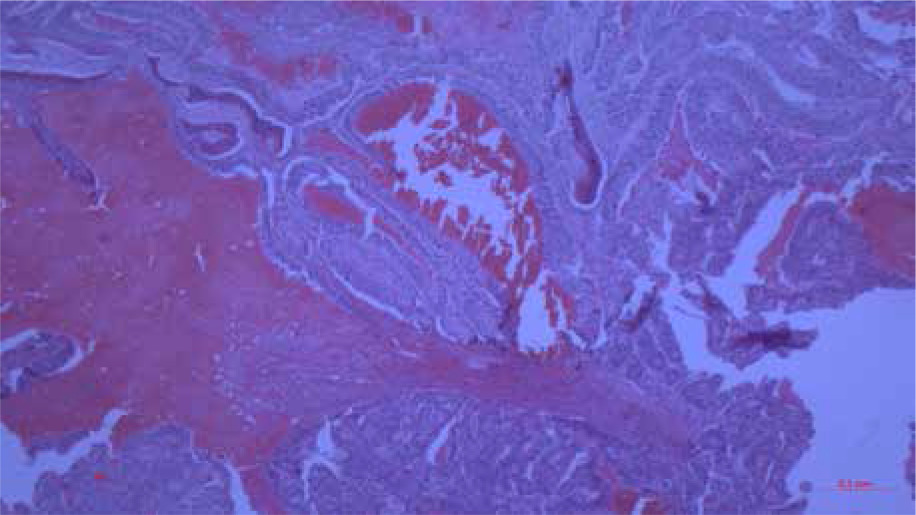
Figure 7
Histological finding of metastatic CRC in the tibia with positive immunohistochemical reaction to CK8 (100×)

Figure 8
Histological finding of metastatic CRC in the tibia with positive immunohistochemical reaction to CK 20 (100×)
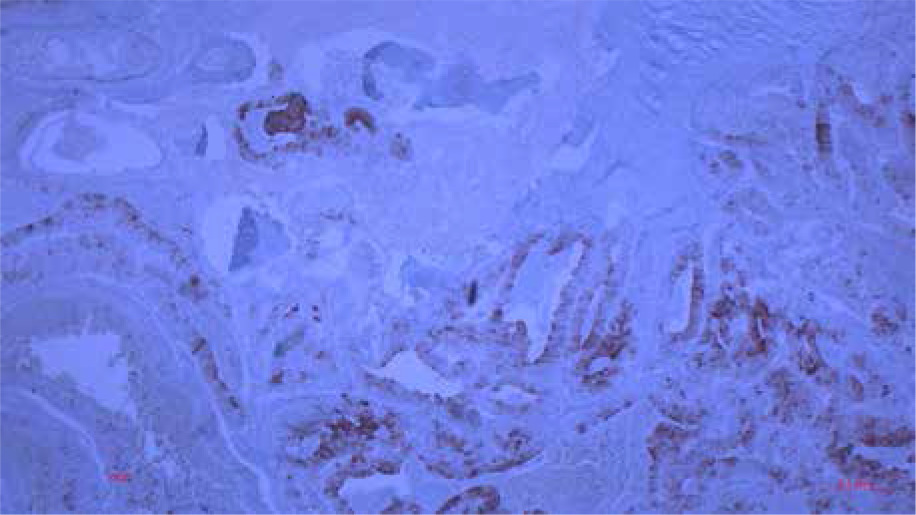
Figure 9
Histological finding of metastatic CRC in the tibia with positive immunohistochemical reaction to BER EP 4 (100×)
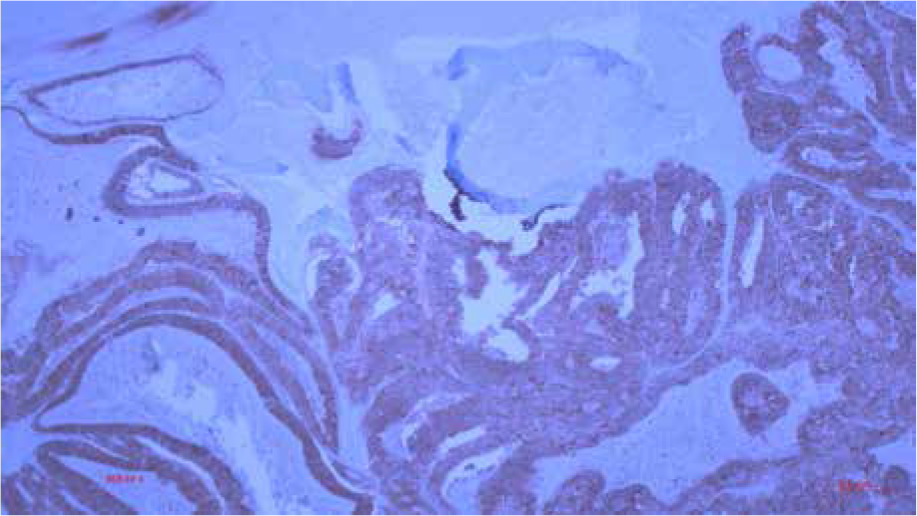
Figure 10
Histological finding of metastatic CRC in the tibia with positive immunohistochemical reaction to CDX2 (100×)
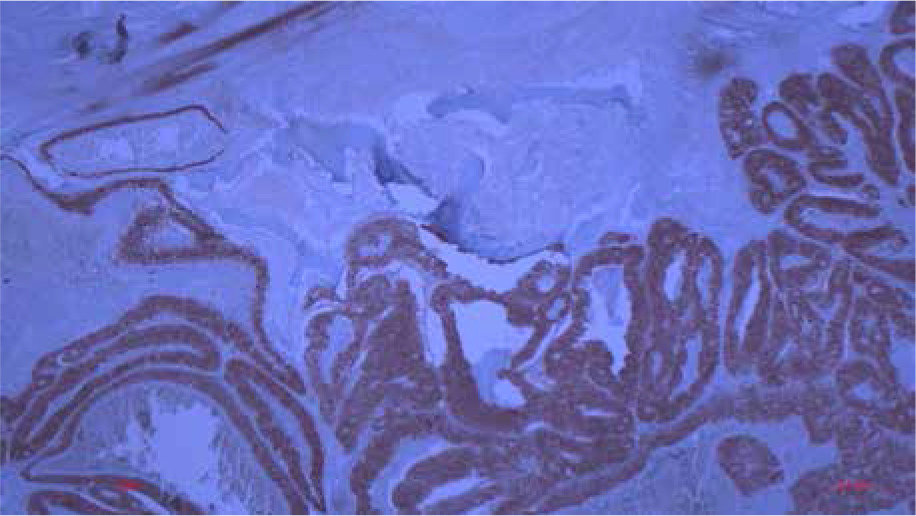
Figure 11
Histological finding of metastatic CRC in the tibia with negative immunohistochemical reaction to CK8 CK7 (100×)
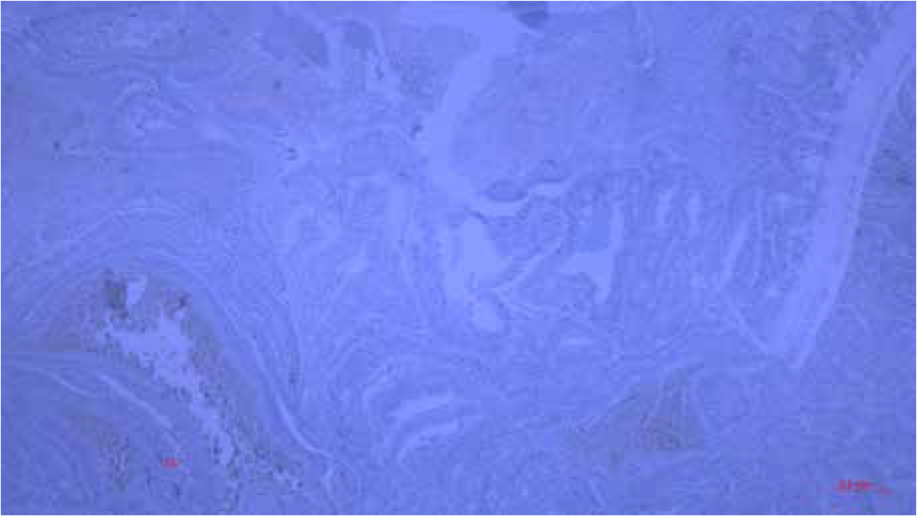
Table I
List of antibodies
Postoperative recovery was uneventful, and the patient was discharged from hospital on the 6th postoperative day after the last surgery.
Literature review results
Three cases of solitary osseous metastases in the tibia from CRC were found in the literature to be adequate for analysis (Table II).
Table II
Solitary tibia metastasis from colorectal cancer. Patient demographics and osseous metastases characteristics
Gender was provided for all patients, and 2 were female. Mean age at diagnosis was 56 ±16 years. The site of the metastases varied in every case, and all parts of the tibia were equally represented. In all the cases the metastases were painful. The mean time from resection of the primary tumour to the diagnosis of the osseous metastases was 13 ±5 months (Table III).
Table III
Diagnosis and management of the CRC with solitary tibial metastasis
Staging of the primary disease was provided for all patients. The stage of the primary disease of 2 cases was classified as Dukes C (TNM stage III), and in one it was Dukes B (TNM stage II). Accordingly, the 2 cases with advanced stage were treated with chemotherapy after the surgical resection of the primary disease.
After a clinical exam, the diagnosis of metastasis was made by scintigraphy in the cases by Chalkidou and Alnajjar, and MR in the case by Kose. In all 3 cases the diagnosis was confirmed by a biopsy. Only Chalkidou reported obtaining a radiography where an osteolytic lesion was seen. Only in Kose’s study a PET-CT was used, which demonstrated hyper-metabolic focuses at the right tibia and paraaortic lymph nodes.
Radiotherapy was the principal treatment for the metastasis in 2 cases; only in the case of Kose et al. chemotherapy was the principal treatment and radiotherapy just a palliative modality added to it. Chemotherapy was eventually used in all 3 cases. Interestingly, in the case of Alnajjar et al. zoledronic acid was administered and an internal fixture laid because of an impending fracture.
All management concepts were successful. In all 3 cases symptom relief was achieved, and CT showed neither new lesions nor progression of the existent tibia lesion and a drop in the CEA levels. All patients were alive at the point of completion of the case report.
Discussion
Breast and lung cancer and, generally speaking, solid tumours are common primary tumours associated with bone metastases [16, 17]. Although CRC itself is unfortunately a frequently encountered entity, bone metastases of CRC are rare. The incidence of bone metastasis is reported in English literature to be between 4.7% and 10.9% in clinical cases and up to 23.7% in autopsy cases [18]. Solitary skeletal metastases are, on the other hand, extremely rare. The first was described by Curling during an autopsy in a patient with rectal cancer and a concomitant radial lesion in 1870 [19]. A retrospective review of CRC patients treated over 25 years performed by Kanthan et al. revealed a 1% incidence of solitary skeletal metastases with sparing of the intraabdominal organs [15]. The typical locations of skeletal metastases from CRC are the vertebrae and pelvis. This predilection has been explained by the most studied intermediary in the spread of CRC – the Batson plexus. The Batson plexus is a venous paravertebral plexus adjacent to the rectum, which drains into the sacral venous plexus. Metastases bypass the portal and caval venous systems in this manner and spread directly to the pelvis and spine. This is why rectal cancers are more frequently associated with bone metastases than other parts of the colon [20].
Long bones are extremely rare the site of solitary CRC metastasis [19]. The development of metastases to long bones has not been explained completely. The communications between the spinal veins in the lumbar region with the iliofemoral venous system may indicate that CRC seeds to the lower extremities in a retrograde fashion [21]. For example, osseous metastases in the foot are most frequently from gastrointestinal cancers [21]. It has been assumed also that the spread is influenced by host factors and tumour factors, including chemotaxis, vascular permeability, and homing cytokine profiles [19].
At the time of writing, in total 8 cases of solitary metastasis to the tibia of CRC have been reported in literature [10–15]. The interval between the treatment of the CRC and the detection of the metastasis varied between 8 and 21 months. Nozue et al. reported a median interval of 16.5 months from the initial diagnosis and operation of CRC to the onset of any osseous metastases in a cohort study consisting of 928 patients [21].
Our case is the 9th case of solitary tibia metastasis from CRC and the first in accessible literature where the symptoms and signs of the metastasis were the presenting feature of CRC. Although in 1 case impending fracture was reported, our case was the first to report a pathological fracture as a result of the metastasis.
The symptoms of tibia metastases can mimic many different benign conditions encountered in the emergency surgical department. Additionally, solitary tibia metastasis in patients with CRC, but also with other solid tumours [16, 19], are extremely rare. Henceforth, clinical awareness among surgeons and emergency department doctors about this clinical entity is not high when seeing oncological patients with painful enlargements of the tibia. An important finding from this literature review is the observation that every tibia metastasis presented with pain. This indicates that all patients presenting with unusual pain in the tibia, especially with CRC in the anamnesis, require a diagnostic work-up.
The most accessible radiological method is regular X-ray. A plain radiograph will show an osteolytic lesion and direct the further work-up. Regarding current literature, there are more possible radiological diagnostic methods. CT and MR are helpful options to further investigate the lesion and assess invasion into surrounding structures [19]. An essential step in the diagnostic work-up is a bone biopsy, which, when performed in all case reports, confirmed the diagnosis, indicating high diagnostic accuracy [10–12].
Currently there is no defined treatment algorithm for this type of metastasis. The reviewed case reports and studies have shown that radiotherapy leads to a significant reduction in pain, which is the chief complaint of such patients [10–12, 16, 19]. An additional, frequently deployed treatment modality is chemotherapy. The administration of zoledronic acid has been reported in only 1 case [11]. Surgical excision of skeletal metastases has shown variable results [19], but the femoral amputation for the tibia metastasis in our case has been potentially curative.
The presence of bone metastases is correlated with poor prognosis [19]. Especially drastic is the difference in the prognosis in the case of multiple compared to solitary skeletal metastases from CRC [15]. Although, according to Kanthan et al., there was no statistical difference found in the 10-year survival rate, 38% of patients with bone only vs. 16% with bone and visceral metastasis were alive at 5-year follow-up [15]. In Bonnheim’s 10-year study of 1406 colorectal cancer cases, 19 patients with isolated osseous metastases had a median survival of 10 months vs. 47 patients with bone and other distant metastases, who had a median survival of 6 months [22].
This is also reflected in the aforementioned case reports – all patients were alive at the point of the manuscript’s completion, in a good clinical state, relying solely on analgesics [10].
The fact that patients with solitary bone metastasis, be it in the tibia or other long bones, have relatively good prognosis obliges surgeons and emergency doctors to bear this clinical entity in mind. Although extremely rare, any surgeon or emergency doctor has to have in mind the possibility that osseous metastases could be the cause of unexplained, atraumatic swelling, haematoma, or pain in the extremities, especially, if they have been diagnosed with CRC or other solid tumours. After an X-ray with a typical radiological pattern, it is recommended that the patient be transferred to the in-patient setting and a thorough radiological work-up conducted. This eventually leads to quick commencement of adequate therapy.
Limitations
This study is strongly limited by the extremely small number of accessible cases in literature. Henceforth, this study can provide only a shallow insight into this clinical entity. There are insufficient data regarding the diagnostic and especially treatment of patients suffering from solitary tibia metastasis from CRC. Because this review included only case reports, we are missing outcome data. The great differences in regard to patient factors like comorbidities and general condition prohibit any sound conclusions. The need for further studies with greater study samples is evident.
Nonetheless, this work provides an overview of solitary tibia metastasis from CRC. The aim of this study is to raise awareness among health-care providers about this entity. We hope to have expanded the list of potential causes of unspecific swelling, haematoma, and pain of the tibia, especially if no history of trauma is present.
Conclusions
Solitary tibia metastasis from CRC is an extremely rare condition, and it is questionable whether every general surgeon encounters a patient with this condition in his lifetime. The spread to the tibia occurs probably retrograde through the iliofemoral veins and is influenced by many factors. The occurrence of atraumatic painful enlargement of the tibia should raise suspicion, and imaging should be conducted because patients with solitary tibia metastasis have a relatively good prognosis.










