
Endoscopists frequently encounter impacted foreign bodies in the oesophagus, which require urgent intervention. Impaction mostly occurs at sites of physiological narrowing and angulations of the oesophagus or at sites of oesophageal stricture or within an oesophageal diverticulum. Dentures, fish, and mutton bolus (steak house syndrome) are common impacted oesophageal foreign bodies in an adult [1]. We present a unique retrieval technique of a large, impacted denture within the mid oesophagus.
An gentleman aged 72 years with no co-morbidity had accidentally ingested an artificial denture 48 h prior to admission and had severe dysphagia and odynophagia. He had no respiratory distress, gastrointestinal bleeding, chest pain or discomfort, cough, or aspiration. At upper gastrointestinal endoscopy, the cricopharynx was grossly oedematous. The denture was dislodged gently using rat tooth forceps and manoeuvred into the stomach. This resulted in surface mucosal ulceration and minimal bleeding. The patient was observed for the next 48 h for any complication. On day 3, a check-up X-ray of the abdomen was taken, confirming its location within the gastric lumen. A repeat endoscopy was attempted, under sedation and airway protection, for denture retrieval after informed consent was obtained explaining the risks involved in its retrieval. At endoscopy, there was a significant reduction in cricopharyngeal oedema.
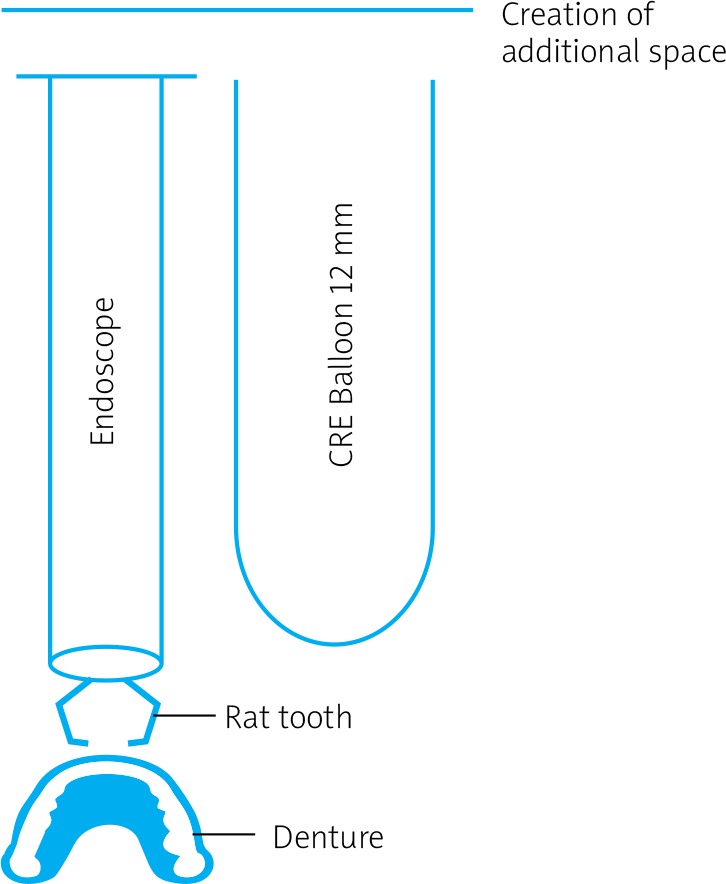
Anticipating problems in retrieving the denture at the cricopharynx, a consensus was reached to create an additional space around the cricopharynx using a controlled radial expansion (CRE) balloon.
In the first instance, the denture was held with rat tooth forceps. A CRE balloon was channelled over a guide wire into the stomach. The balloon was placed in close proximity to the endoscope and slightly proximal to the forceps grasping the denture, and both were steered proximally under fluoroscopy guidance. At the cricopharynx, the CRE was inflated to 12 mm, thus creating an additional space, which helped in retrieving the denture with ease (Figure 1). Post procedure was uneventful, and the patient was discharged a day later.
Impacted foreign bodies within the oesophagus may lie free within the lumen or can be buried deep in the mucosal or muscular layer of the oesophagus. The latter leads to mucosal oedema, and ulceration progressing to penetration and perforation. Other complications include mediastinitis, para- or retropharyngeal abscess, tracheal compression, empyema, perforation, and aortoesophageal fistula [2, 3].
Rigid and flexible oesophagogastroscopes have been used for the removal of sharp and large foreign bodies. The former have greater success rates of retrieval at 94–100% with lower rates of complication such as perforation (0.34%). With flexible scopes the success rates are low, at 76 and 98.5%, and with slightly higher rates of perforation (0–0.5%) [4, 5]. Retrieval of a foreign body has been attempted using lower oesophageal sphincter relaxants like benzodiazepines, calcium channel blockers, and glucagon [6]. The results are often not encouraging. Occasionally, long-standing impacted dentures may even require a thoracotomy [7]. For sharp pointed objects, grasping forceps, polypectomy snares, baskets, retrieval nets, transparent caps, and latex rubber hoods have been used to prevent mucosal injury [8]. The use of balloon devices like CREs and Fogarty balloons for the removal of oesophageal foreign bodies has also been described in the literature [9, 10].
The present case highlights an acute presentation of a large, impacted denture in the upper oesophagus.
In conclusion, in the presence of an oedematous cricopharynx, it is safer to dislodge the foreign body into the stomach. A watchful wait for 48 to 72 h causes a significant reduction of cricopharyngeal oedema. An additional space can be created at the non-oedematous cricopharynx for a large foreign body, such as dentures, by using a scope-guided CRE balloon.










