
A 62-year-old male patient was referred to our endoscopic centre for qualification for an endoscopic re-reseciton in 2016. The reason was suspicion of infiltrating cancer in the margins of ascending colon polyp in histopathology. The polyp had 10 mm diameter and was removed during the first colonoscopy in the other endoscopic centre. Before the control examination, the patient had additional imaging examinations, which showed the T1 stage of disease. Our endoscopic examination showed an incomplete resected polyp in the ascending colon (Figure 1 A). After marking the margins of the lesion with a tattoo, an endoscopic full-thickness resection was planned. The procedure was performed in anaesthetic analgosedation using a PCF-H190D colonoscope with Olympus Evis Exera III CV/CLV-190 tower. After the introduction of the colonoscope and localisation of the lesion, the margin was determined using the included marking probe (APC ERBE 20 W) (Figure 1 B). After mount the FTRD System® (Ovesco Endoscopy, Tübingen, Germany), a resection of the lesion was performed (Figures 1 C–E). After removing the FTRD System, the resection site was revised. The treatment went without complications. During the subsequent days of hospitalisation, no gastrointestinal bleeding or perforation symptoms were observed. The tightness of the over-the-scope clip (OTSC) in the control colonoscopy was completed, and the patient was discharged home. Because of the uncertain result of one of the margins of the obtained material, a planned right-sided hemicolectomy was performed. In the histopathological examination of the postoperative material, an inflammatory polyp with granulation was found at the location of the OTSC clip, without the presence of neoplastic infiltration. No metastases were found in the seventeen lymph nodes collected intra-operatively. In the follow-up colonoscopy, performed 6 months after the procedure, relapse was not seen in the remaining part of the colon. Surgical anastomosis was normal.
Figure 1
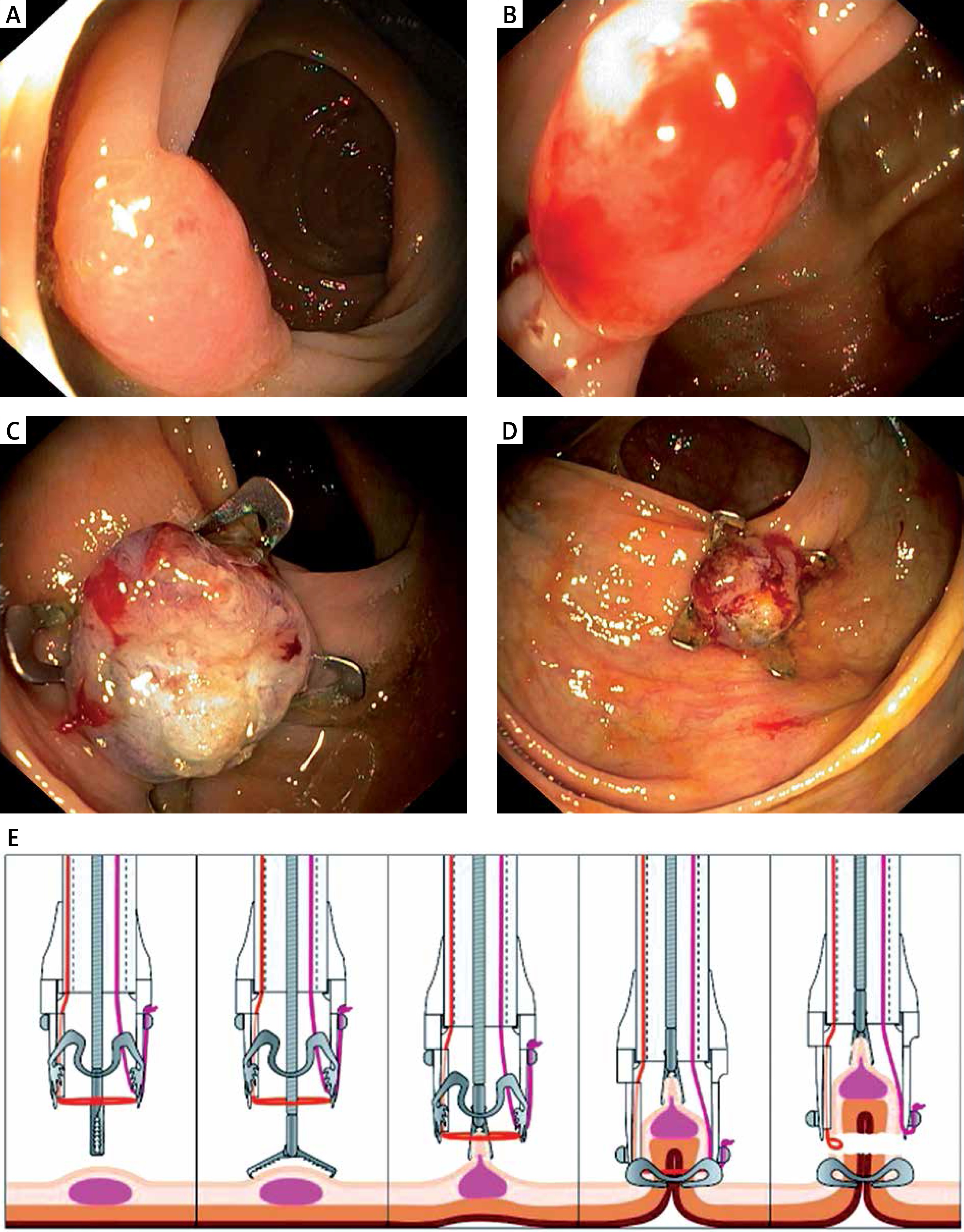
A – Non-complete resection of ascending colon polyp with high-grade dysplasia, with a focal presence of cancer, B – marking the margins of the lesion, C – the lesion site with over-the-scope clip after the full-thickness resection (FTRD, Ovesco Endoscopy, Tübingen, Germany), D – the lesion site with overthe- scope clip after the full-thickness resection (FTRD, Ovesco Endoscopy, Tübingen, Germany), E – FTRD System® (full thickness resection device, Ovesco Endoscopy, Tübingen, Germany), www.ovesco.com
Advanced endoscopic procedures such as endoscopic mucosal resection (EMR) or submucosal dissection (ESD) are used in the case of extensive superficial wall layers of the gastrointestinal tract [1, 2]. The above-mentioned endoscopic techniques may be difficult to perform due to high risk of perforation, and they are sometimes insufficient to achieve curative resection (R0) in the case of non-lifting signs, subepithelial tumours (SETs), advanced local fibrosis, tumours with deep infiltration, incomplete resection of the intestinal adenomas and post-resection recurrences, as well as adenomas with problematic localisation like the diverticulum or appendix [3–5]. Endoscopic full-thickness resection (EFTR) with an OTSC device (full-thickness resection device – FTRD) can be alternative method for EMR, ESD and classical surgical procedure in selected cases [3]. In the present case FTRD was an effective and safe method in deep resection of lesions, even with carcinoma infiltration.










