
Introduction
It is generally accepted that colon cancer is the most commonly diagnosed gastrointestinal cancer and a major public health problem. As revealed by studies, the clinical outcomes of the patients, especially those with lymph node-positive status, are still unsatisfactory [1, 2]. It is worth noting that about 20% of the diagnoses are made in the metastatic stage of the disease, where the percentage of 5-year overall survival is less than 15%. However, the prognoses are not satisfactory even in the case of patients with primary tumours [3–5].
Therefore, the identification of novel approaches to describe patients from the high-risk group, particularly in the context of the clinical outcomes, has become a major challenge.
Snail1 is a zinc-finger transcription factor, which plays a role in colorectal cancer development by silencing E-cadherin expression and inducing epithelial-to-mesenchymal transition (EMT). Therefore, in colon cancer patients, enhanced levels of Snail1 are usually associated with poor clinical outcome, probably due to down-regulation of E-cadherin expression [6–8].
Aim
The current study investigated the expression of Snail1 protein in colon adenocarcinoma samples to assess its prognostic significance by correlating its expression with the clinicopathological variables and survival of Caucasian patients.
Material and methods
Tissue samples
The study was conducted on formalin-fixed and paraffin-embedded colon adenocarcinoma samples archived in the files of the Department of Pathomorphology in Zabrze (Poland). Tissue specimens were received from 97 colon adenocarcinoma patients who underwent surgical resection on surgical clinics in 2012.
The exclusion criteria were as follows: (1) history of previous malignant disease, (2) familial adenomatous polyposis, (3) inflammatory bowel disease, (4) preoperative anti-cancer treatment, and (5) evidence of distant metastasis. The clinicopathological characteristics obtained from the medical records were as follows: age, gender, location of tumour, grade of tumour differentiation, depth of invasion, lymph node metastasis, operation record, treatment record, recurrence, and vital status at the last follow-up date.
The colon adenocarcinoma specimens belonged to 48 men and 49 women (mean age: 68 years; range: 33–89 years). Tumours were located in the proximal part of the colon in 50 (51.5%) cases and in the distal part of the colon in 47 (48.45%) cases. Three levels of differentiation were used to classify the grading as follows: well differentiated (G1), 14 (14.43%) cases; moderately differentiated (G2), 52 (53.61%) cases; and poorly differentiated (G3), 31 (31.96%) cases (Table I).
Table I
Demographic and clinical characteristics of colon adenocarcinoma patients included in the study (n = 97)
Immunohistochemical staining
For the immunohistochemical studies the paraffin-embedded specimens were cut into 4-µm-thick sections, fixed on Polysine slides, deparaffinised in xylene, and rehydrated through a graded series of alcohol. To retrieve the antigenicity, the tissue sections were treated twice with microwaves in a 10-mM citrate buffer (pH 6.0) for 8 min each. Subsequently, sections were incubated with rabbit polyclonal antibody to SNAI1 (final dilution 1 : 500) (GeneTex; cat. number GTX100754). For visualisation of protein expression, the sections were treated with a BrightVision detection system and Permanent AP Red Kit (Zytomed). Mayer’s haematoxylin was used to counterstain the nuclei.
Semi-quantitative analysis of Snail1 expression in colorectal adenocarcinoma samples
The scores were assigned separately for the stained area and for the intensity of the immunohistochemical reaction. Quantification connected to the stained area of the tissue section was performed as follows: (1) < 33% of cells showed immunoreaction, (2) 33–66% of the cells had positive reaction to Snail1, and (3) > 66% of the cells were positive. The intensity of the immunohistochemical reaction was quantified as follows: (1) absent or weak, (2) moderate, and (3) strong. Each tissue section was characterised by a final grade derived from the multiplication of the stained area and the intensity of the staining. The Snail1 expression was considered to be: absent/low for grade 1; moderate for grades 2, 3, and 4; and strong for grades 6 and 9.
Survival analysis
Survival analysis was conducted in 97 patients. The survival curves were generated using the Kaplan-Meier method. The overall survival (OS) was defined as the length of time between surgery and death. The follow-up period was 60 months. Patients alive were censored at 5 years.
Statistical analysis
Statistical analyses were conducted using Statistica 9.1 (StatSoft, Poland). The clinical characteristics of the patients in relation to vimentin immunoreactivity were assessed by performing the Kruskal-Wallis test and U Mann-Whitney test. Additionally, using Spearman’s rank correlation coefficient, the relationship between the immunoexpression of GRP94 and age, grade of tumour differentiation, and size of primary tumour was assessed. The Kaplan-Meier method was used to study survival curves, and the long-rank test was used to compute differences between the curves.
Results
To investigate the clinicopathological and prognostic roles of Snail1 expression, the immunohistochemical analysis was performed in colon tumour tissues and adjacent non- pathological mucosa. It should be noted that only trace expression of this protein was revealed in adjacent non-tumour colorectal mucosa, whereas high expression was demonstrated in well, moderately, and poorly differentiated tumours (Figure 1). Among the 97 samples, 11 (11.34%) showed a weak immunohistochemical reaction, 35 (36.08%) demonstrated moderate immunoreactivity, and 51 (52.58%) revealed strong expression.
Figure 1
Immunohistochemical expression of Snail1 in colon adenocarcinoma patients according to intensity of immunohistochemical reaction
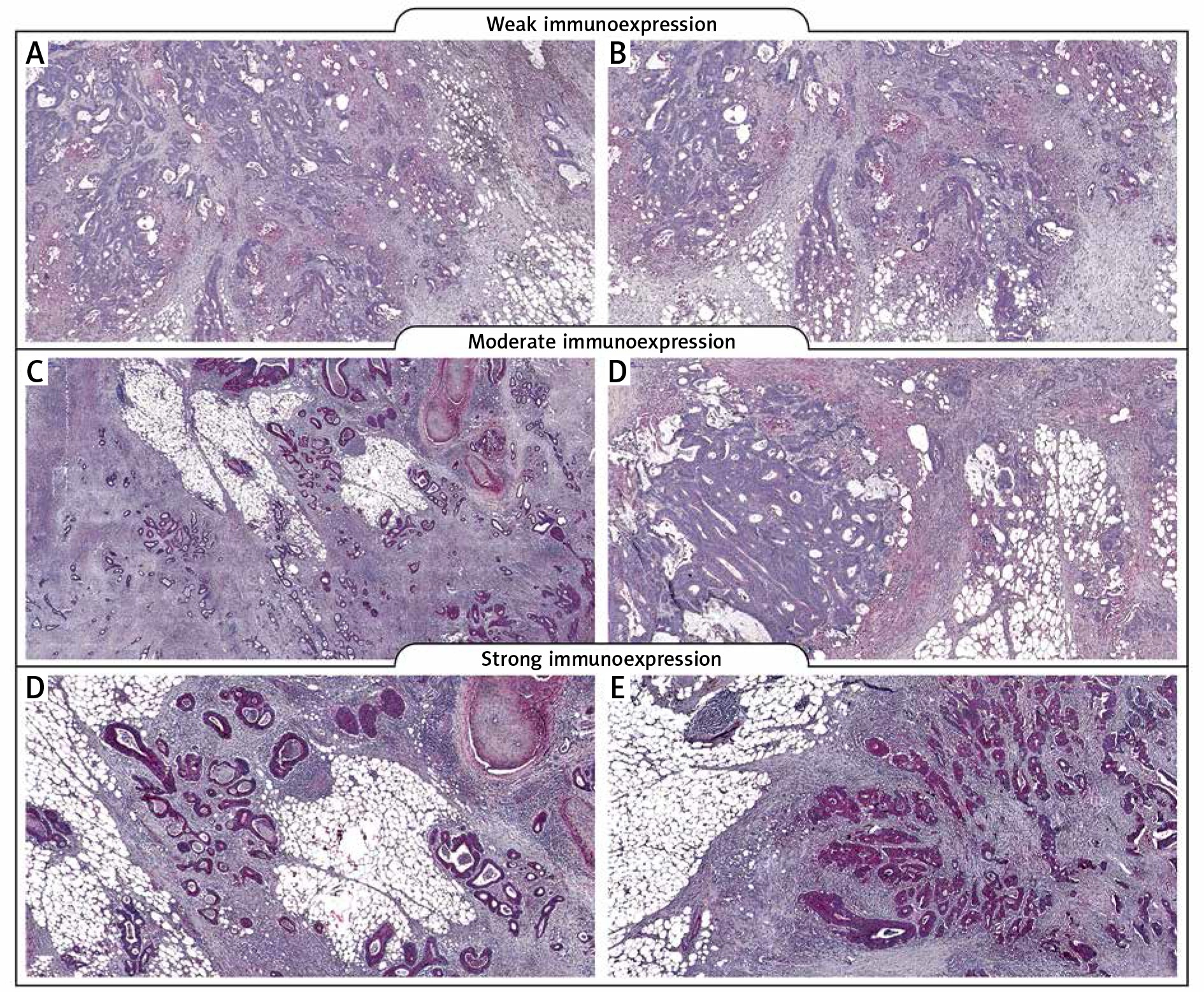
The relationships between the Snail1 levels and each clinicopathological parameter are summarised in Table II. As demonstrated, the level of the Snail1 immunohistochemical reactivity was correlated with the grade of the histological differentiation (H [2.97] = 37.949; p < 0.001). A strong expression of Snail1 protein was detected more frequently in patients with G3 tumours than in patients with G1 tumours. Moreover, a significant difference was also detected between the patients with G1 tumour and G2. In the G2 patients a strong reactivity was described more frequently. The statistical evaluation of Snail1 immunoexpression according to age, sex, tumour location, and depth of invasion revealed no significant difference among these variables (all p > 0.05; Table II).
Table II
Correlations between Snail1 immunoexpression and clinicopathological characteristics in colon adenocarcinoma patients
The Kaplan-Meier survival analysis showed that the overall survival rate in the group of patients with a low expression level of Snail1 was significantly longer than that for patients with a moderate or strong level of Snail1 immunoreactivity (p < 0.001; Figure 2). The 5-year overall survival for patients with a low, moderate, or strong level of Snail1 immunoexpression was 100%, 25.7%, and 2%, respectively. The Snail1-moderate patients had an average survival time of 44.886 months (95% CI: 40.855–48.916), whereas the Snail1-strong expression groups had an average survival time of 21.706 months (95% CI: 17.863–25.549) (Table III). In the univariate analysis the grade of tumour differentiation and Snail1 immunoexpression were found to be significantly associated with reduced 5-year survival. Moreover, a multivariate analysis demonstrated that grade of tumour differentiation (HR = 2.150; 95% CI: 1.380–3.349, p = 0.001) and Snail1 expression (HR = 3.901; 95% CI: 2.436–6.247, p < 0.001) were the independent risk factors for worse survival (Table IV).
Figure 2
Kaplan-Meier survival curves of colon adenocarcinoma patients with weak, moderate, and strong expression of Snail1 protein; follow- up period = 60 months
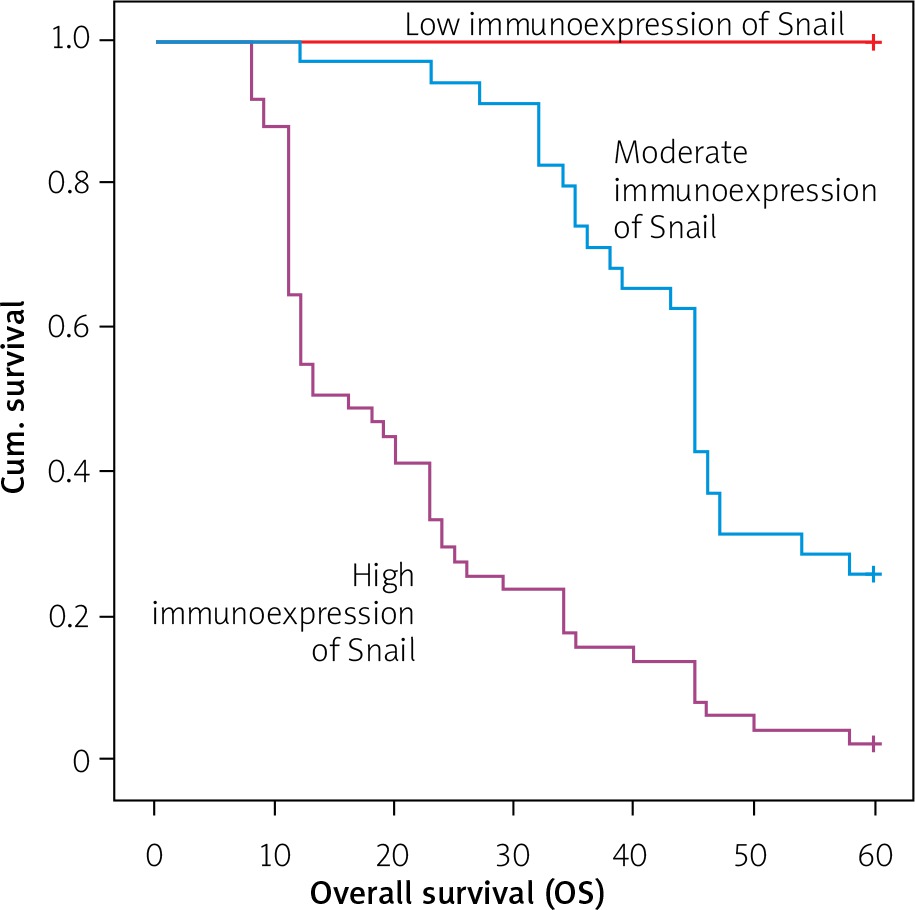
Table III
Means and medians for survival time of colon adenocarcinoma patients according to Snail1 immunoexpression
Table IV
Multivariate analyses of various prognostic parameters in colon adenocarcinoma patients using Cox- regression analyses
Discussion
The results of our study demonstrate that in comparison to samples of non-tumour colon mucosa, the samples of colon cancer were characterized by high levels of Snail1 immunoreactivity. Moreover, the high levels of vimentin immunoexpression were demonstrated to be associated with malignancy-related clinicopathological factors and 5-year overall survival among Caucasian patients. It should be pointed out that the high immunoexpression of Snail1 was significantly related to advanced histological tumour grade. The Kruskal-Wallis test showed a statistical difference between the patients with G1 tumours and those with G2 tumours, and between the patients with G1 tumours and those with G3 tumours. In both cases, patients with G1 tumours were described by a low level of vimentin immunoexpression (p < 0.001). As revealed by the studies during colorectal cancerogenesis, the adenoma is the first stage exhibiting Snail1 expression, which is inversely correlated with expression of E-cadherin [7]. This finding is in agreement with the statement that Snail1 acts as a transcriptional repressor of CDH1. It is well demonstrated that repression of CDH1 is a consequence of molecular reaction cascade, during which a major role is played by interactions with regions containing the consensus core sequence (CAGGTC), a motif that is a subset of E-box (CANNTG) [9, 10]. The expression of Snail1 in adenoma tissue suggests that the EMT process promoting cancer metastasis is already active in precancerous lesions. Studies with the use of transgenic mouse models such as HER-2 and PyMT have revealed that tumour cells may disseminate in morphologically benign hyperplastic lesions [11]. It should be stressed here that in the case of colon tissue, Snail1 expression has also been revealed in normal mucosa in close vicinity to the tumour lesions. Interestingly, some differences between non-pathological tissue and cancer tissue have been demonstrated at the subcellular level, where the shift of the protein to the cytoplasm with mixed cytoplasmic and nuclear or pure cytoplasmic expression has been detected [12]. Regarding Snail1 expression in colorectal mucosa with no specific pathological changes, some published results suggest that Snail1 is not associated with malignant transformation only. In non-pathological mucosa, this factor may be involved in the maintenance of homeostasis by regulation of processes at the cellular level such as proliferation, differentiation, and apoptosis [12].
Moreover, up-regulation of Snail1 expression has been reported to promote regional and distant lymph node metastasis [13, 14]. Snail1 expression as a marker for lymph node metastasis has also been reported in the case of breast cancer and oesophageal squamous carcinoma [14–16]. Some authors revealed that about 77% of colon cancer samples display Snail1 immunostaining in the stroma, especially in the stromal cells with fibroblast-like phenotype [17–19]. Expression of this factor in the stroma will indicate how many cells possess the ability to escape from the primary tumour mass and how many cells may invade the basal lamina to colonize distant target organs [20]. Therefore, the presence of Snail1 immunoreactive cells in the stroma may serve as prognostic marker in patients with colon cancer. It is worth noting that intratumoural injection with Snail1-specific monoclonal antibody inhibits tumour growth and metastasis followed by an increased number of stromal tumour-infiltrating lymphocytes (TILs). Snail1 immunoreactivity in tumour stroma is related to distant metastasis and lower specific survival of patients [18]. Importantly, this correlation was also detected in stage I and II, which are known to display a variable prognosis. The capability to predict recurrence at these stages would be important from a clinical point of view because markers for them have not yet been identified. Thus, the expression of Snail1 would help to distinguish patients with an unfavourable clinical outcome and would be applicable for chemotherapy, which is not a treatment commonly used in the early stages of colorectal tumours [18]. It is worth noting that no association between Snail1 expression and clinical parameters has been revealed in adenocarcinomas of the upper gastrointestinal tract [21]. Probably, there are other more powerful mechanisms, which are implicated in EMT triggering during colon cancer development, e.g. factors associated with the Wnt signalling pathway. Larriba et al. revealed that Wnt signalling and Snail1 may be interconnected by multiple positive loops, possibly adding to the robustness of both [22].










