
The most common cause of benign stenosis in the large intestine is the anastomotic stricture, which occurs in 5–20% after colorectal resection [1, 2]. The term anastomotic stricture refers to the narrowing of the intestine, which results in clinical symptoms of complete or partial intestinal obstruction [3]. The predisposing factors for this serious complication are not clearly understood, but anastomotic leakage, preoperative radiation, and ischaemia due to excessive tension in the anastomosis correlate with increased incidence [4]. Anastomotic strictures often concern interventions in the middle or low rectum, and they usually self-improve over time [5]. Nevertheless, persistent strictures will require intervention such as endoscopic- or fluoroscopy-guided dilatation, stenting, reoperation, or incision of the stricture with diathermy during endoscopy [6]. Anastomotic strictures in the early postoperative period are rarely reported in the bibliography, and they are usually observed at a median 5–12 months following surgery [7]. Early anastomotic stricture is defined as a stricture that requires intervention within 6 weeks of gastrointestinal anastomosis creation [8]. We present the case of a female patient who developed an anastomotic stricture following right colectomy for colon cancer and on the 14th postoperative day. After a failed endoscopy, she underwent anastomotic dilatation under fluoroscopic guidance with alleviation of symptoms.
A female patient, 65 years old, with a history of dyslipidaemia, arterial hypertension, and coronary disease with angioplasty, was referred to our hospital because of an ascending colon cancer that was found during colonoscopy for anaemia investigation. The patient underwent scheduled right colectomy, and a hand-sutured side-to-side ileocolic anastomosis to the distal transverse colon was performed. On the 5th postoperative day, the patient presented signs of intestinal obstruction with decreased bowel sounds in auscultation, abdominal distension, bile vomiting, and inability to pass gas and stool. Laboratory exams were normal, and an abdominal X-ray revealed gas fluid levels as well as distension of the small intestine loops. Intestinal obstruction and high output of the Levin tube persisted, so the patient underwent an abdominal computed tomography (CT) scan that revealed a transition point in the level of the anastomosis and minimum passage of the oral contrast to the large intestine (Figures 1 A, B). The daily gastrointestinal fluid losses were over 1.5 l, so water and electrolyte imbalances were continuously replenished and from the 7th postoperative day the patient was nutritionally supported with total parenteral nutrition. The persistence of intestinal obstruction was probably due to anastomotic stricture, with kinking or creation of a narrow anastomosis. On the 14th postoperative day, a colonoscopy was performed in order to dilate the ileocolic anastomosis and manage the intestinal obstruction. The patient underwent 2 colonoscopies without success because of a 360° turn of the sigmoid colon and hence inability to proximally pass the scope. As a salvage option, before the reoperation, the passage of a guidewire under fluoroscopic guidance from the anus was decided. A stiff guidewire with straight tip and length of 260 cm was used initially in combination with an angiographic 5 Fr catheter that was used for contrast injection. The sigmoid 360° turn was overpassed and then an angled stiff type guidewire was placed over the angiography catheter in order to pass through the ileocolic anastomosis (Figures 1 C, D). The contrast injection showed continuity with the ileum, and the angled-type guidewire was able to proximally pass the anastomosis. An Amplatz super stiff guidewire was then placed in order to achieve better stability to pass a larger catheter through the anastomosis (Figure 1 E). Finally, a levin tube 18 Fr was placed through the Amplatz guidewire, proximally to the ileocolic anastomosis, and was sutured in the perianal area (Figures 2 A, B). The small intestine was decongested, and the Levin tube led to the straightening and dilatation of the ileocolic anastomosis. A CT scan was performed subsequently to exclude possible intestinal injury and to confirm the correct position of the tube (Figures 2 C, D). The tube remained in place for 2 days and the patient started feeding. After removal of the tube the gastrointestinal tract was fully mobilized and the patient was discharged in good condition. In 2 years of follow-up, the patient remains free of disease without any symptoms of obstruction.
Figure 1
A – Anastomotic ileocolic stricture in the distal transverse colon (blue arrow). B – Transition point in the level of the ileocolic anastomosis (red arrow). C – 360° turn of the sigmoid colon overpassed with the Amplatz catheter. D – Guidewire passed through the ileocolic anastomosis, with contrast in the ileum. E – A stiff catheter is passed over the guidewire for better stability
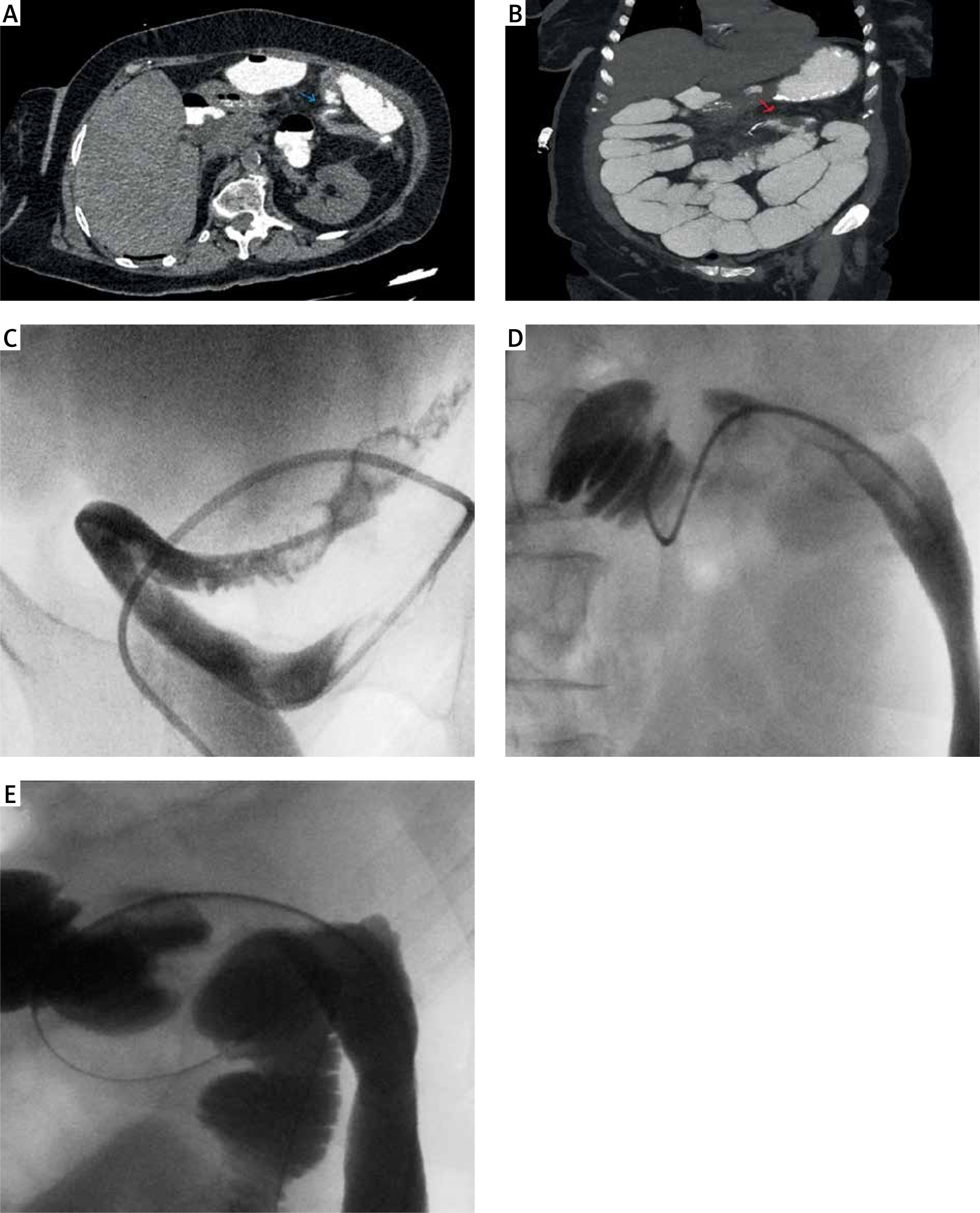
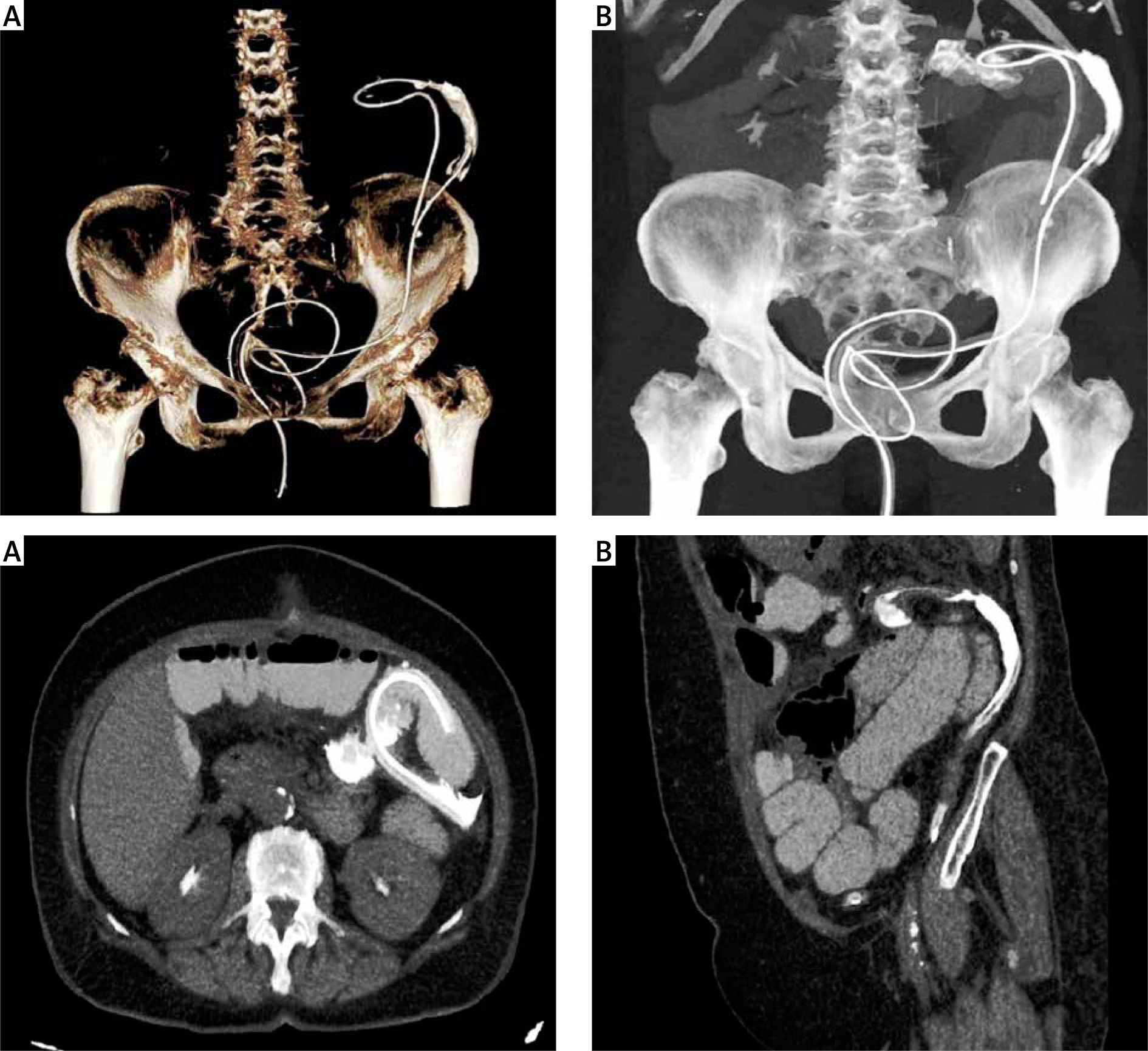
Figure 2
A, B - Final position of the Levin tube showing the difficulty in the sigmoid colon and the passage proximal the anastomosis. C - Levin position with straightening and dilatation of the anastomosis. D - Levin in the descending colon
The incidence of anastomotic stricture ranges from 3 to 30%, and only 5% will present with symptoms of intestinal obstruction [9]. The time of presence is usually 5–12 months following colorectal surgery, and anastomotic strictures in the early postoperative period are rarely reported in the bibliography. These strictures have a different aetiology and are usually related with bad technique, oedema, or kinking of the anastomosis. This complication is serious because the water deficit, the electrolyte imbalances, and the malnourishment are burdens for a safe reoperation, as the morbidity raises. Previously, reoperation with a new anastomosis was the only choice available, although with high morbidity and difficulty because of the adhesions [3]. Nowadays, reoperation is the last option for resolution of an anastomotic stricture. The optimal and safest method, according to several studies, is endoscopic management and balloon dilatation [6]. Besides endoscopic management, dilatation under fluoroscopic guidance is also reported with similar results [10]. In our case the patient had twice undergone colonoscopy unsuccessfully, with inability to pass a 360° turn of the sigmoid. The only option available, in order to avoid reoperation, was dilatation under fluoroscopic guidance.
The intervention in a newly created Anastomosis during the healing phase is of high risk because the mechanical tension during endoscopy and the air inflation may lead to disruption of the anastomosis. The maximum anastomotic strength is obtained at least 4 weeks after surgery, and an early intervention is quite risky; hence, there is scarce evidence in the bibliography concening the management of an anastomotic stricture in the early postoperative period [11]. The healing phase in the gastrointestinal tract consists of 3 phases: lag, proliferative, and remodelling. Initially, the anastomotic strength depends on the suturing. The proliferative phase from day 4 to day 14 is when a large amount of collagen is produced. According to a study by Jonsson et al., in the 3rd postoperative day the suture strength is reduced to 15% of the initial strength, before it begins to increase on day 4 [12]. Finally, the remodelling phase starts from day 14 until 4 weeks for the small intestine and 4 months for the large intestine, when the maturation of the collagen leads to maximum strength [11]. It is also reported in studies that the production of collagenase in the lag phase is limited to the small intestine. As a result, ileocolic anastomoses obtain maximum strength faster in the early postoperative period and are more durable after an early endoscopy [8]. Therefore, endoscopic dilatation of an early anastomotic stricture should take place after the 14th postoperative day, when the proliferative phase ends and collagen strength is obtained. When endoscopy fails, dilatation under fluoroscopic guidance should always be considered as a salvage option because it is a minimally invasive method and the morbidity of a reoperation is avoided.










