
Introduction
Acute cholecystitis represents a common general surgical emergency and is one of the most frequent complications of gallstones requiring inpatient hospital admission. Definitive treatment requires cholecystectomy to prevent further gallstone-related complications. Operative intervention during the initial hospital admission has been associated with improved patient outcomes with decreased long-term complications, shorter overall length of stay, and reduced overall healthcare costs [1–4]. However, in critically unwell patients who may not be able to tolerate surgery, percutaneous cholecystostomy represents a management option to control sepsis. This procedure involves a drainage tube being inserted through the skin into the gallbladder, usually under image guidance. This procedure aims to drain the gallbladder and relieve sepsis in those patients who are not considered suitable for emergency cholecystectomy, and it provides a clinical improvement in over 85% of patients within 48–72 h of the intervention [5]. Percutaneous cholecystostomy is particularly utilised in high-risk patients such as those being treated in intensive care or the elderly. Increasing age significantly reduces the likelihood of emergency cholecystectomy being undertaken [6, 7], in part due to the reduced physiological reserve of these individuals and the associated increase in peri-operative risks. This can lead to increased utilisation of percutaneous cholecystostomy in elderly patients who are deemed unfit for cholecystectomy.
The use of percutaneous cholecystostomy in critically unwell patients is reflected in the Tokyo Guidelines for management of acute cholecystitis [8, 9], which recommend that in patients with evidence of organ dysfunction (grade III cholecystitis) percutaneous cholecystostomy can be utilised to drain the gallbladder and control sepsis prior to interval cholecystectomy. However, only around 40% of patients receiving percutaneous cholecystostomy will go on to receive definitive cholecystectomy within 1 year [10]. Of those patients treated with percutaneous cholecystostomy alone, up to 46% develop further episodes of cholecystitis within 3 years [11].
Aim
This systematic review and meta-analysis aimed to evaluate the outcomes of elderly patients treated with percutaneous cholecystostomy versus treatment with emergent cholecystectomy.
Material and methods
An electronic literature search was undertaken using the Embase, Medline, and Web of Science databases up to May 2020. The search terms ‘cholecystostomy’ and ‘percutaneous cholecystostomy’ and the Medical Subject Heading (MeSH) ‘cholecystostomy’ (MeSH) were used in combination with the Boolean operators AND or OR. Three authors (ST, CL, DK) performed the electronic search independently in May 2020. The electronic search was supplemented by a hand-search of published abstracts from relevant meetings. The reference lists of articles obtained were also searched to identify further relevant citations. Abstracts of the articles identified by the electronic search were scrutinised to determine their suitability for inclusion in the pooled analysis.
Publications were included if they were case-matched controlled or comparative studies in which patients underwent percutaneous cholecystostomy or emergency cholecystectomy for acute cholecystitis. Studies were excluded if they were non-comparative or investigated alternative management strategies such as delayed cholecystectomy. Because this review aimed to specifically investigate the utilisation of percutaneous cholecystostomy in elderly patients, studies were also excluded if the mean age in the percutaneous cholecystostomy group was below 65 years.
Outcome measures
Primary outcome measures were mortality (in-hospital and 30-day) and overall morbidity (defined as a complication developing within 30 days of the procedure – either percutaneous cholecystostomy or cholecystectomy). Secondary outcome measures were length of hospital stay and readmission rate.
Statistical analysis
Data from eligible studies was entered into a computerized spreadsheet for analysis. Statistical analysis was performed using StatsDirect 3.2.9 (StatsDirect, Altrincham, UK). Percutaneous cholecystostomy was utilised as the reference group. Weighted mean difference (WMD) was calculated for the effect of emergency cholecystectomy on continuous variables. Pooled odds ratios (POR) were calculated for the effect of emergency cholecystectomy on discrete variables. All pooled outcome measures were determined using random-effects models as described by DerSimonian Laird [12]. Heterogeneity among trials was assessed by means of the Cochran’s Q statistic, a null hypothesis in which p < 0.05 is taken to indicate the presence of significant heterogeneity [13]. The Egger test was used to assess the funnel plot for significant asymmetry as an indication of possible publication or other biases.
Results
The literature search identified 19 case-matched control or comparative studies and one randomised control trial, which were included for analysis [14–33]. Figure 1 shows the PRISMA flowchart for the literature search. In total there were 689,874 patients included, with 28,241 patients receiving percutaneous cholecystostomy. There were 662,327 patients treated by other means in the comparison group, with 661,633 undergoing cholecystectomy and 694 having been treated conservatively in one study, which also included patients managed with emergency cholecystectomy [17].
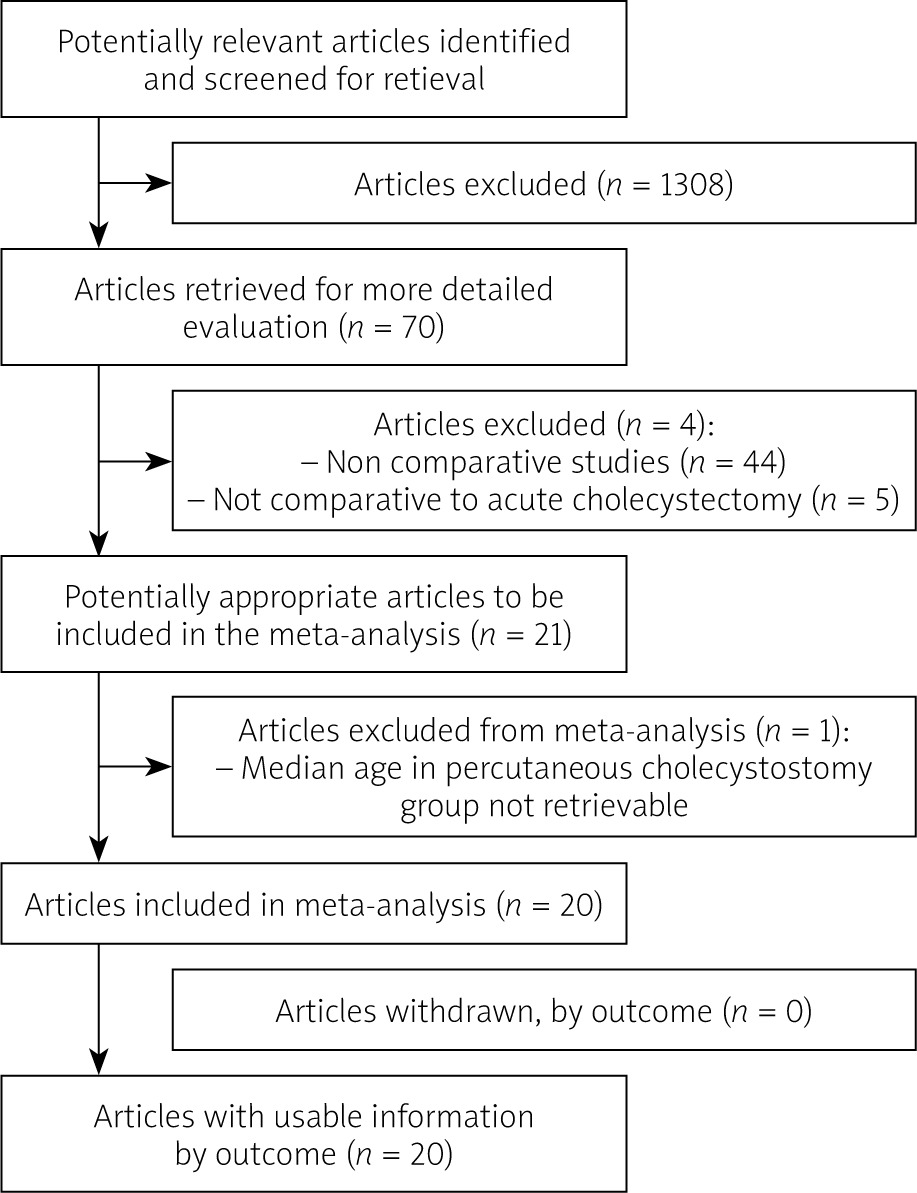
Table I describes patient demographics in each included study. Table II shows the results from the individual studies for the clinical outcome measures evaluated in this pooled analysis.
Table I
Details of patient demographics for each included study
Table II
Outcome details for each included study
Mortality
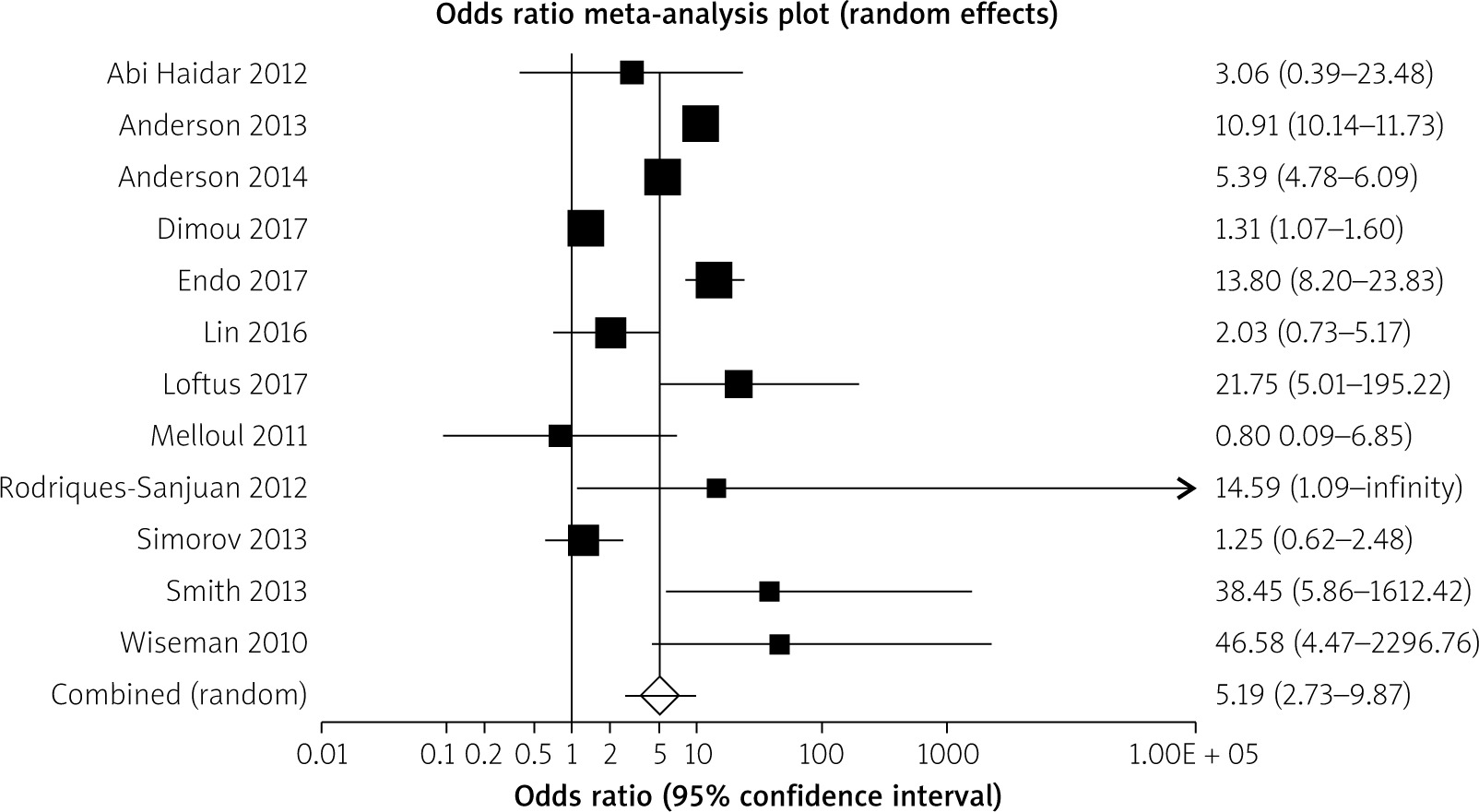
The incidence of mortality was demonstrated by 17 studies [14–23, 25–27, 29–31, 33]. The utilisation of percutaneous cholecystostomy was associated with a significant increase in mortality (POR = 4.85; 95% CI: 1.02–7.30; p = 0.0001) (Figure 2). There was proof of statistical heterogeneity (Cochran Q = 698.55; p < 0.0001; I2 = 97.3%), but no evidence of bias (Egger = –2.67; p = 0.41).
Overall morbidity
Overall morbidity was studied in 13 studies [14–18, 20, 23–25, 29–31, 33]. There was no significant difference in overall morbidity between percutaneous cholecystostomy and emergency cholecystectomy (POR = 0.92; 95% CI: 0.45–1.98; p = 0.83). There was proof of statistical heterogeneity (Cochran Q = 237.02; p < 0.0001; I2 = 93,7%), but no evidence of bias (Egger = –2.06; p = 0.33).
Secondary outcome measures
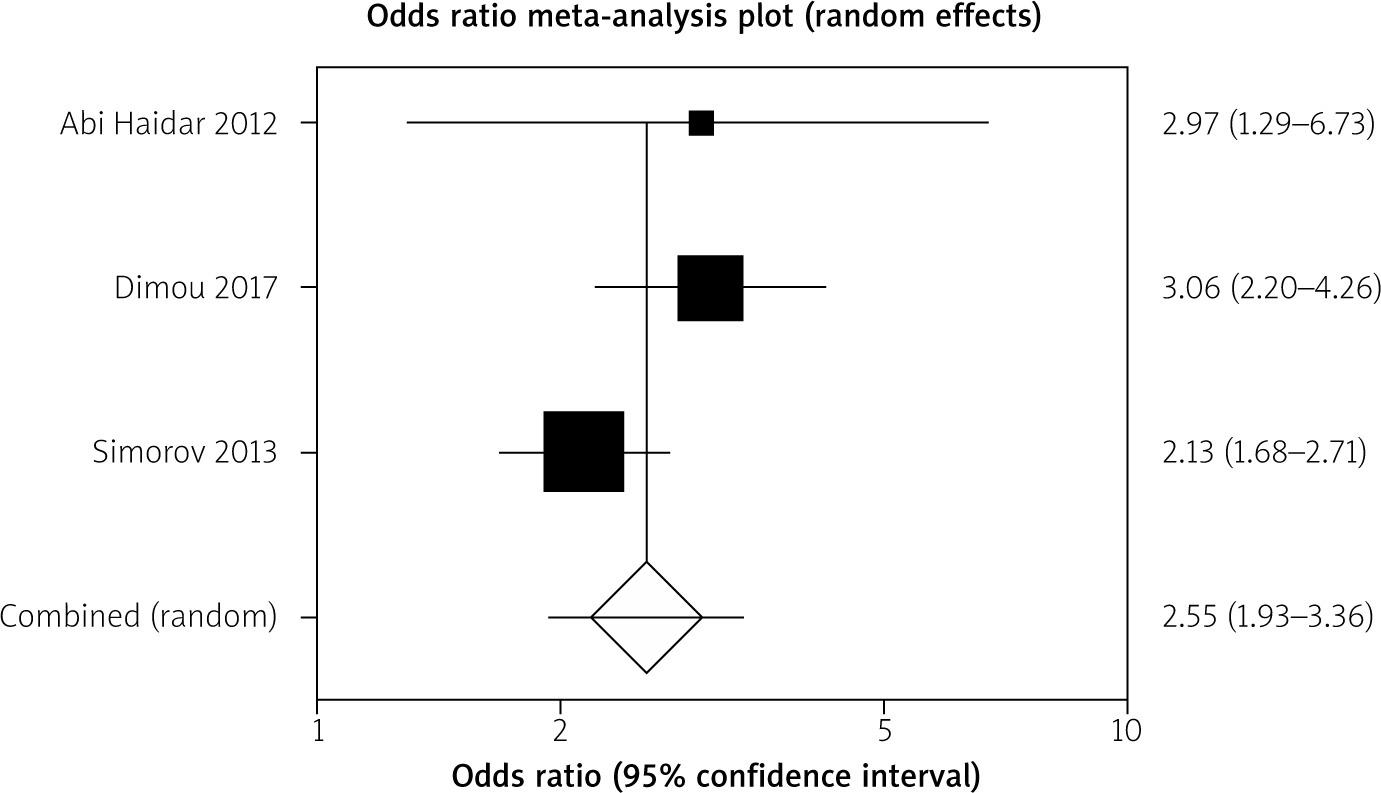
Three studies stated rate of readmission [14, 17, 23]. Percutaneous cholecystostomy was associated with a significantly increased rate of readmission (POR = 2.95; 95% CI: 2.21–3.87; p < 0.0001) (Figure 3). There was no proof of significant heterogeneity (Cochran Q 10.44; p = 0.21; I2 = 33.2%).
Figure 3
Percutaneous cholecystostomy associated with significantly increased rate of readmission (POR = 2.95, 95% CI: 2.21–3.87)
Eleven studies reported length of stay [14–24]. There was no significant difference in length of stay between the two groups (pooled weighted mean difference: 0.47; 95% CI: –1.74 to 2.92; p = 0.64). There was evidence of heterogeneity (Cochran Q = 18654.23; p < 0.0001; I2 = 100%), but no proof of bias (Egger = –18.97; p = 0.21).
Discussion
This systematic review and meta-analysis highlights that patients treated with percutaneous cholecystostomy appear to have increased mortality and readmission rates relative to those treated with cholecystectomy on index admission with acute cholecystitis.
Previous studies identified that undertaking cholecystectomy for elderly patients during initial hospital admission prevents further episodes of gallstone-related disease, reduces readmission rates, and is associated with lower overall healthcare costs [34]. The study by Riall et al. identified that 38% of elderly patients who did not receive cholecystectomy on primary hospital admission would be re-admitted with gallstone-related readmission within 2 years, compared to a 4% readmission rate for those undergoing cholecystectomy [34].
In order to extend the benefits of acute cholecystectomy to critically unwell patients who are deemed unfit for surgery, previous studies have suggested utilising percutaneous cholecystostomy as a ‘bridging-procedure’ prior to early cholecystectomy within a few days [35, 36]. This management strategy allows sepsis to be resolved by decompression of the gallbladder using percutaneous cholecystostomy, and one study reported clinical resolution of toxaemia within 24 h in 85% of patients following percutaneous cholecystostomy placement [35]. Following resolution of sepsis, patients may be more likely to be considered as candidates for surgery.
The laparoscopic approach for cholecystectomy is known to provide significant advantages to patients in terms post-operative recovery [37]. There have been concerns that undertaking delayed cholecystectomy following the prior placement of a percutaneous cholecystostomy can be associated with increased conversion from laparoscopic to open surgery, with some previous studies reporting conversion rates as high as 32–43% [38–40]. However, when utilising percutaneous cholecystostomy as a bridge to surgery, the aforementioned studies reported laparoscopic completion rates of 87.7% and 93.5% when cholecystectomy was completed within 5 days of PC placement [35, 36].
To date, there has been no published randomised controlled trials (RCT) that have compared the utilisation of percutaneous cholecystostomy with conservative management in acute cholecystitis. There is only one, recently published, RCT that compared percutaneous cholecystostomy with laparoscopic cholecystectomy in the emergency setting [31]. The present pooled analysis is based mainly upon non-randomised data, and therefore there are important limitations that must be considered in the interpretation of the results gained. The Tokyo guidelines recommend the utilisation of percutaneous cholecystostomy only in patients who have severe grade III cholecystitis with evidence of organ dysfunction [8, 9]. Those patients receiving percutaneous cholecystostomy may have more been more significantly unwell during the acute episode than those deemed suitable for surgical treatment with cholecystectomy. This factor may have been partially responsible for the increased rates of mortality with percutaneous cholecystostomy identified in the current pooled analysis.
The multicentre RCT was concluded early after a planned interim analysis, because laparoscopic cholecystectomy compared with percutaneous catheter drainage was proven to reduce the rate of major complications. The rate of death did not differ between the laparoscopic cholecystectomy and percutaneous catheter drainage group [31]. This general outcome is the exact opposite of the pooled analysis findings of the included studies in this review. The early termination of the RCT and the subsequent small number of patients in comparison with the other observational studies may be responsible for this discrepancy in the results. One other limitation in comparing the results of this RCT with the current meta-analysis is the different definition of mortality (1 year versus 30 days). However, this study provides a more robust evaluation of the potential benefits of laparoscopic cholecystectomy in high-risk patients with acute cholecystitis.
Only one study in the present pooled analysis included patients who had been managed conservatively (n = 694) as well as those managed with cholecystectomy (n = 995) in the reference group [25]. This formed part of a propensity-matched analysis with and without percutaneous cholecystostomy tube placement in grade III cholecystitis. It was not possible to separate the outcome data for patients who underwent cholecystectomy and those managed by conservative means for this study. This study provided important information regarding readmission rates following percutaneous cholecystostomy or alternative management strategies. Therefore, it was decided to include this study in the pooled analysis despite the fact that not all patients in the control group had received cholecystectomy.
It is difficult to determine the relative effectiveness of PC with or without delayed cholecystectomy compared to early cholecystectomy due to selection bias in favour of patients treated with PC. Other limitations of the current analysis include the fact that there was a significant amount of statistical heterogeneity in the analysis for mortality, morbidity, and hospital stay. This is likely to have been secondary to the variations in study populations for articles included in this pooled analysis.
Conclusions
This pooled analysis has established that patients treated with percutaneous cholecystostomy appear to have increased mortality and readmission rates compared to those managed with cholecystectomy. However, the utilisation of percutaneous cholecystostomy remains a valuable clinical tool in patients who are unfit for surgical intervention. Where possible, percutaneous cholecystostomy should be considered as a ‘bridge to surgery’, with cholecystectomy being undertaken following resolution of sepsis and patient stabilisation.










