








Introduction
Nursing care rationing is a global problem that can be a real threat to the health and lives of patients. The term was coined in 2006 by a nurse Beatrice J. Kalisch [1]. To date, it has not been standardized, is rarely analyzed, and does not have its precise definition [2].
Rationing of care occurs when nursing care has been omitted in whole or in part due to various external factors [3]. This phenomenon is primarily due to a lack of time among the staff, which is caused by staff overload, e.g. due to too many patients per nurse, new treatment options or low skill levels. Factors that contribute to the rationing of nursing care are labor resources, material resources and teamwork [4]. Nursing staff and patients report that the nursing care received by patients is not optimal when the number of staff is insufficient [5]. Research shows that the main activity that gets rationed is the patients’ oral hygiene and the communication with patients and their families [6]. In addition, communication problems translate into, e.g. inadequate patient education, the solution to which is to increase staff numbers and financial resources at the facilities in question, as well as for the staff to regularly evaluate activities that have been started and remain unfinished [7].
In turn, limited financial resources are the reason for not hiring enough nursing staff. Also, working in wards with a high number of patient deaths translates into a deterioration of nurses’ emotional health and the occurrence of chronic fatigue syndrome. It has a significant impact on the efficiency of the work they do and the omission of some activities they perform [8]. Overlooking some responsibilities is also due to low levels of motivation, which directly affects an employee’s productivity. There are three types of motivation factors: organizational ones directly related to the work performed, social, and personal, which relate to the individual characteristics of an employee. All of them are essential for doing effective work [9].
The consequences of nursing care rationing are not fully understood but skipping any activity affects the patients’ health negatively and results in medical errors that pose a direct threat to their health [4]. Several studies have shown that there is a link between nursing staff skipping care and the occurrence of treatment errors, the onset of infections, bedsores or falls among patients. It was also checked whether there was an association between the omission of nursing care and mortality but no such relationship was proven [5].
Due to the prevalence of the phenomenon in question, there is a need to study it and make potential changes to improve the situation. Standardized tools should be used in the research. The best known tool is the BERNCA care rationing questionnaire created by Schubert. It consists of 32 questions that make it possible to determine the frequency of nursing care rationing. The higher the score obtained, the greater the rationing of care [3].
The RANCARE (Rationing – Missed Nursing Care: an International and Multidimensional Problem) research project funded by the European Union under the Horizon 2020 Framework Program was conducted with the participation of 27 countries until 2019. Its main goal was to discuss the rationing of nursing care worldwide, which directly translates into patient safety. According to the findings, the reduction of the frequency of the phenomenon is to be achieved through cooperation between countries and the creation of a unified definition [4].
Aim of the work
The aim of the work was to investigate the incidence of care rationing by medical personnel and analyze the activities that are most often limited in patient care.
Material and methods
A total of 217 nurse practitioners participated in the study. The inclusion criteria consisted of working in an intensive care unit and consenting to participate in the study. The analysis used an original questionnaire including questions about education, main place of work, number of hours worked per month, feelings toward devoting adequate time to patient care, and reason for rationing care, as well as standardized questionnaires: BERNCA, the Generalized Self-Efficacy Scale (GSES) and the Health Behavior Inventory (HBI).
Statistical validity of the observed phenomena was verified as a=0.05. Test probability p (p-value) was determined and then compared to the validity level and when p<0.05, statistical validity of respective relationships or differences was demonstrated.
Results
A total of 217 nurse practitioners participated in the study. The mean age was 39.9 years, SD=11.09 years, and the majority were women (N=149; 68.66%), urban residents (N=126; 58%) who had completed a bachelor’s degree (N=113; 52.07%), a master’s degree (N=69; 31.79%) or a medical college (N=35; 16.14%). Respondents were most likely to have additional education in anesthesiology and intensive care (N=98; 45.16%), followed by those with no additional education (N=64; 29.49%), those who have completed a course in blood drawing (N=24; 11.05%), BLS (N=17; 7.83%) and other courses such as wound care, EKG (N=14; 6.47%). Most worked at one workplace (N=113; 52.07%), followed by two workplaces (N=87; 40.09%) and three workplaces (N=17; 7.84%). It was observed that respondents most often work twelve-hour days (N=167; 76.95%), men are more likely to work more jobs (p=0.296) but the place of work is not related to gender (p=0.421).
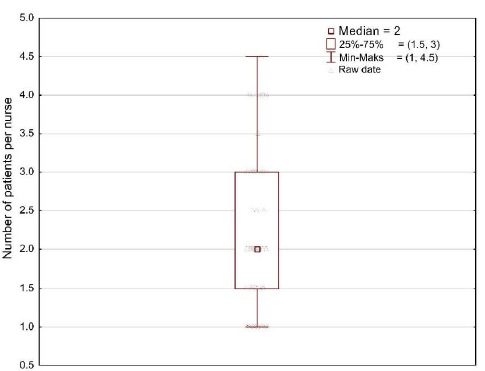
On average, there are 2 patients per nurse while 50% of those surveyed care for more than one but fewer than four. The results are statistically significant p<0.05 (Figure 1).
According to the survey, women are slightly more satisfied with the quality of their patient care than men, and they devote sufficient time to their patients (Table 1).
Table 1
Relationship between satisfaction with the quality of patient care, adequate amount of time devoted to care and the respondents’ gender
The survey showed that the most frequently cited reason for rationing of care by medical personnel is the lack of sufficient staff and additional activities performed outside of nursing activities (Table 2).
Table 2
Reasons for rationing nursing care
| Causes | N | % |
|---|---|---|
| Lack of staff | 104 | 47.92 |
| Additional activities | 35 | 16.13 |
| Professional burnout | 34 | 15.67 |
| Lack of equipment | 15 | 6.91 |
| Work organization | 12 | 5.53 |
| Lack of knowledge | 11 | 5.07 |
| Work system | 6 | 2.77 |
The study found that women rationed nursing care to a greater extent than men (Table 3); informing the patient about planned tests or treatment was the most frequently rationed activity (N=14; 6.47%), and skin care was the least frequently or never rationed one (N=163; 75.11%) (Table 4).
Table 3
Analysis of the results of the BERNCA-R Rationing of Care Questionnaire
| Variable | Rationing nursing care | ||||
|---|---|---|---|---|---|
| N | Average | Min. | Max. | SD | |
| BERNCA-R | 217 | 1.91 | 0.66 | 4.00 | 0.73 |
| K | 149 | 1.96 | 0.80 | 4.00 | 0.77 |
| M | 68 | 1.81 | 0.66 | 3.00 | 0.66 |
Table 4
Analysis of rationed activities
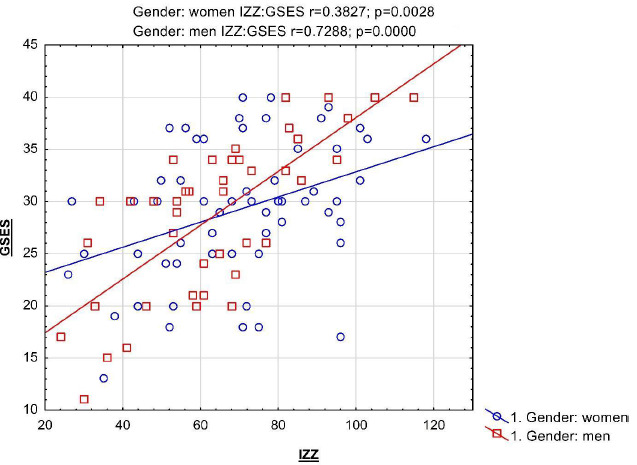
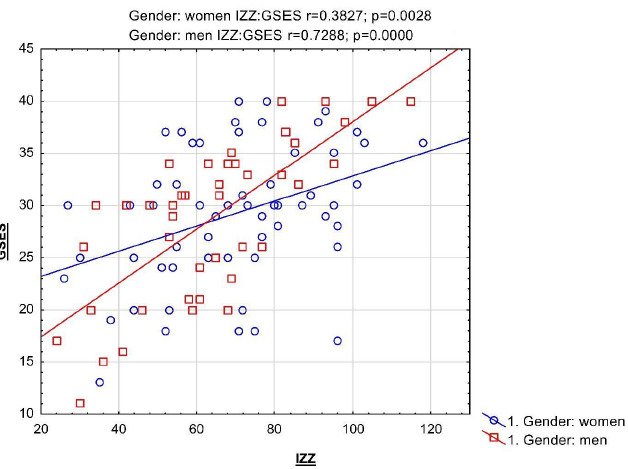
As health behaviors increase among the respondents, the incidence of self-efficacy in the activity performed increases as well (Figure 2).
According to the responses given by the surveyed medical personnel and according to the BERNCA-R questionnaire, as the number of patients per nurse increases, the rationing of nursing care visibly increases too (Figure 3).
According to the responses given by the surveyed medical personnel and according to the BERNCA-R questionnaire, as the number of patients per nurse increases, the rationing of nursing care visibly increases too (Figure 3).
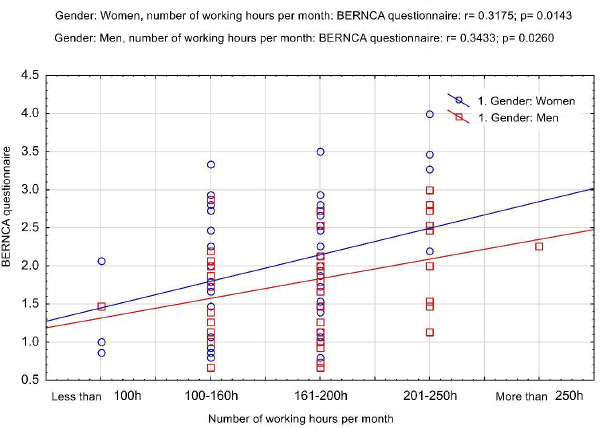
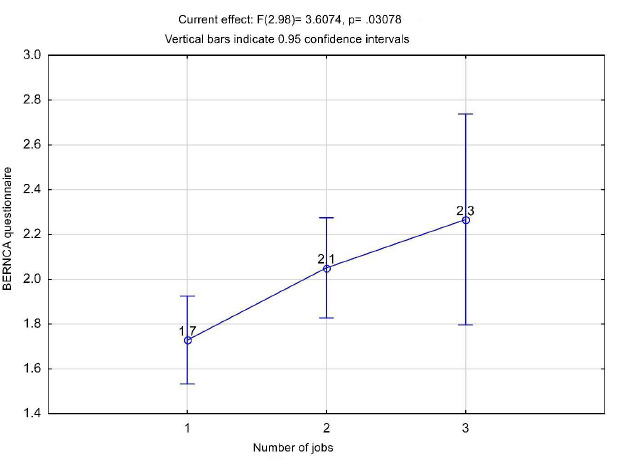
Statistically significant differences in care rationing were observed with regard to the number of jobs and the number of hours worked per month. As they increase, nursing care rationing visibly intensifies too, and the more jobs there are, the more care is rationed (p=0.032). It was also demonstrated that there is a statistically significant difference between the rationing of care when a respondent has one job (the lowest level of rationing) and the other groups. There is no significant difference in care rationing between those with 2 and 3 jobs, although rationing increases with the number of jobs (Figure 4 and Figure 5).
Statistically significant differences in care rationing were observed with regard to the number of jobs and the number of hours worked per month. As they increase, nursing care rationing visibly intensifies too, and the more jobs there are, the more care is rationed (p=0.032). It was also demonstrated that there is a statistically significant difference between the rationing of care when a respondent has one job (the lowest level of rationing) and the other groups. There is no significant difference in care rationing between those with 2 and 3 jobs, although rationing increases with the number of jobs (Figure 4 and Figure 5).
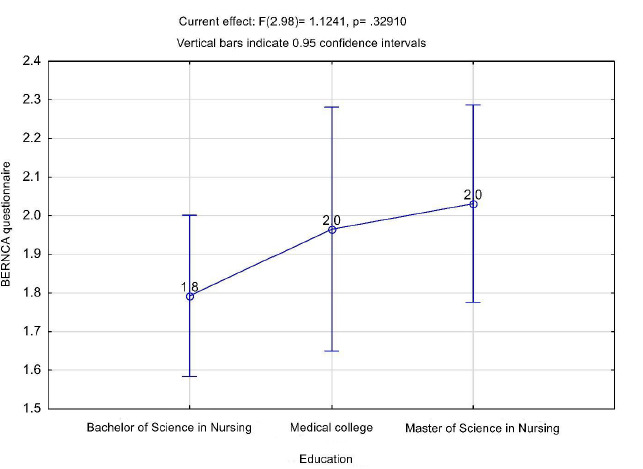
The survey did not show that care rationing was significantly related to the education of the respondents, however, it was observed that the BERNCA questionnaire score increases with higher education (Figure 6).
The relationship between the amount of time spent on non-nursing activities and nursing care rationing was also analyzed. Figure 7 shows the actual relationship between the studied variables by gender of the respondents. An outlier was observed in the women’s group, which is why Spearman’s coefficients were additionally determined and the observed relationship was confirmed. It is similar in both gender groups and shows that, as time for extra activities increases, the rate of care rationing increases too (Table 5). In addition, differences are observed in the BERNCA-R care rationing level but they are not statistically significant between the male and female groups.
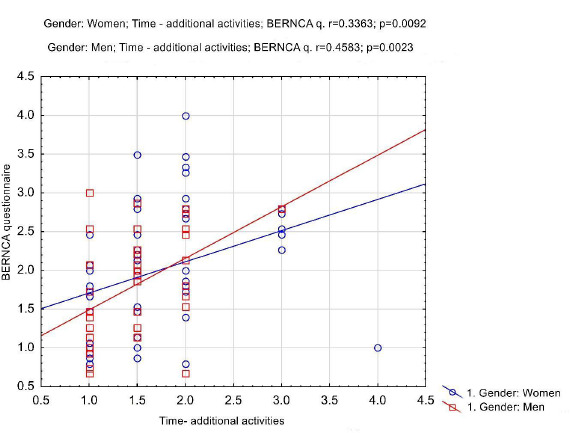
Table 5
Analysis of the relationship between the performance of extra activities and care rationing
Discussion
The problem of nursing care rationing is very common regardless of the department in which a nurse works. Nursing care rationing means omitting or discontinuing care altogether [10]. Nurses who ration care contribute to consequences that lead to risks to patient safety [11].
According to research, the main reasons for this phenomenon include insufficient human and material resources, as well as interpersonal communication problems [12]. The phenomenon of care rationing is widespread around the world, affecting some 30-40% of the staff [13].
Increased rationing of nursing care may also be driven by the decisions of the institution’s managers and dictated by cost-effectiveness with consideration of the impact of rationing on patients’ health. Despite staffing shortages, managers ensure that nurses will continue to provide full care [14].
According to Rooddehghan, degrees of nursing care rationing are important in terms of developing, among other things, a health care system structure that is appropriate especially from an ethical perspective. This procedure is very important as it greatly affects the health and even the lives of the patients, as well as demonstrates the values prevalent in a society. Therefore, further research in this area is needed to minimize the impact and omission of tasks [15].
According to the research conducted for this study, nurses ration care more often when there are more than an acceptable number of patients under their care than the staff with an adequate number of patients under their care. Rochefort et al. obtained similar results in their analyses. They demonstrated that staffing shortages and an unfavorable work environment are reasons to increase nursing care rationing [16]. In turn, Mantovan has proved that nurses postpone tasks or reduce the quality of activities performed to prevent or reduce rationing. Similar conclusions were also reached by Xiaowen, who observed that the lack of staff resources has a significant impact on intensifying the degree of nursing care rationing, making it difficult for a hospital to provide quality care to patients [17], which was also confirmed by the results presented here.
All the analyses discussed above also found that women are more likely than men to ration care, and the most frequently rationed activity was informing the patient about planned tests or treatment. In contrast, activities such as skin care were rarely or never reduced. In addition, it was shown that, as health behaviors increase among the surveyed personnel, their self-efficacy increases as well. Low self-efficacy causes anxiety, among other things, while high self-efficacy is advantageous in terms of taking on challenges and achieving success [18]. This may prove that people with a high sense of self-efficacy are willing to engage in health behaviors, which is in line with the results of the study.
The most frequently mentioned reasons for care rationing by medical staff include insufficient staffing and additional activities performed outside of nursing activities. This is borne out by a number of studies that demonstrate that care rationing by the nursing staff is primarily due to their multitasking. This means that too many responsibilities with too few staff negatively impact the level of care provided. Fatemeh has demonstrated that the incidence of adverse events increased with high workload [12,19]. Therefore, it can be concluded that with more jobs and the associated increased number of working hours per month, there is an increase in care rationing, which is most likely due to nurses being overworked. These conclusions were confirmed in the analyses conducted for this study. In addition, nurses work in an environment that is severely physically and mentally taxing. They are continuously in contact with people who need care and require assistance. They also usually work in several workplaces. As a result, they often become exhausted, which can lead to professional burnout. Both of these factors reduce their ability to work, as well as the motivation to continue working, which significantly increases the risk of medical errors [20].
According to a study conducted in Texas, a large proportion of staff admitted that they had made a mistake due to fatigue, which could potentially jeopardize patient safety [21,22]. According to the responses obtained from the personnel surveyed for this study, a nurse working in an Intensive Care Unit cares for 2 patients on average but half of the respondents work at several workplaces and rationing of nursing care apparently increases as the number of workplaces increases. The study also proved that staff who spend more time doing extra activities also increase the degree of care rationing. Therefore, nursing staff should not have to work in several places, have no outsourced extra tasks, and have an adequate number of patients under their care for whom they would be able to provide adequate care.
According to the results of our own study, gender does not significantly impact care rationing. The same results were obtained in the analyses conducted by Młynarska who additionally proved that seniority has no effect on the level of nursing care rationing either [23]. Unfortunately, this phenomenon was not studied in the research conducted for this paper, which needs to be completed in subsequent analyses. Instead, the focus was on the level of education of those working in intensive care units and the impact of their education on the degree of nursing care rationing. Education was shown not to be significantly associated with care omission but those with higher education were rationing care to a minor degree. This may be due to the fact that people with higher education may have more extra tasks to perform, which translates into increased care rationing [1,11].
Conclusions
Women are slightly more satisfied with the quality of patient care they provide than men, and they devote sufficient time to their charges.
Women rationed nursing care more than men, and informing patients about tests or treatment was the most common task to be rationed.
As the number of patients per nurse increases, the level of nursing care rationing increases as well.
As the number of working hours and the number of workplaces increase, the level of nursing care rationing increases as well.
Those with higher education are more likely to ration care.
The level of care rationing increases as the number of additional activities performed increases.