
Introduction
Colorectal cancer (CRC) represents the third most common cancer and the second leading cause of cancer-related death worldwide [1]. The CRC is responsible for significant incidence rates of global cancer-related morbidity and morbidity. Although colon screening programs have reduced the incidence rates in several parts of the world, the mortality is still rising in some parts of the world [2, 3]. Many risk factors have been implicated in the aetiology of CRC, including dietary [4], environmental [5], and genetic factors [6].
CRC is highly preventable if powerful prevention strategies are implemented, including lifestyle changes, screening the at-risk population, and widespread public primary prevention strategies. Substantial progress in CRC prevention can be strengthened by the design of new screening policies, positioning the accessible CRC screening models to enhance the outcomes while ensuring sensible expenditure of assets [7].
There is a lack of epidemiological data on CRC, although early studies indicated it as the commonest cancer among men and the third most common cancer among women in Saudi Arabia. The disease tends to affect the younger generation, particularly women. Most cases present with advanced stages of the disease, denoting the lack of screening or public awareness towards early detection [8, 9]. Several studies from Saudi Arabia have claimed a low level of awareness towards CRC prevention, screening, and early diagnosis [10, 11], which revealed patients seeking help at the late stages of the disease.
Aim
Consequently, the present study aimed to determine the patterns and stages of colon cancer presentation in Northern Saudi Arabia.
Material and methods
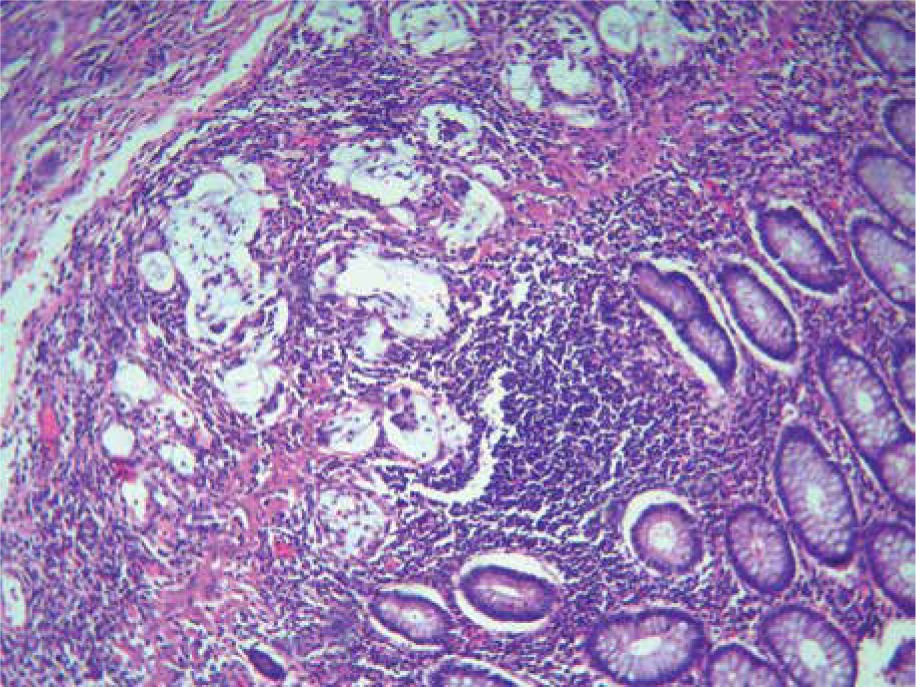
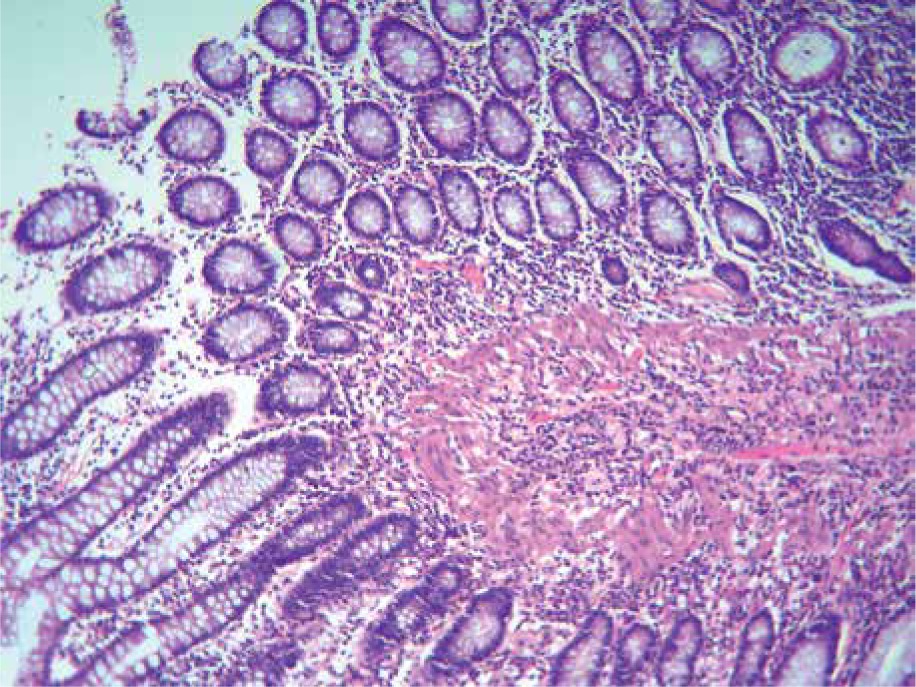
Retrieved data and tissue blocks related to 50 colorectal patients from King Khalid Hospital, Hai’l province, Northern Saudi Arabia were used in the study. The sample represented all available colorectal specimens (full coverage cancer cases within 10 years). The retrieved data included a full histopathology report, gender, and age. All tissues were retrieved in the form of formalin-fixed paraffin wax processed blocks. The tissues were found to be obtained in the form of colonoscopy or/and biopsy. All tissue blocks were sectioned and stained using haematoxylin and eosin method to confirm the prior diagnosis. The histopathological assessment process role was achieved by offering a pathological classification category considering the histological type of malignancy and differentiation stage. The categorization of conventional adenocarcinoma was achieved by glandular formation. Invasive carcinoma is categorized by invading cancer cells through mascularis mucosa into the submucosa, as well as the presence of desmoplastic reactions. Grading of moderately differentiated adenocarcinoma was stated when glandular formation accounted for 50–95%. Poorly differentiated adenocarcinoma was stated when glandular construction accounted for < 50%, and most lesions revealed concrete patterns.
Statistical analysis
All retrieved variables were entered into the computer software Statistical Package for Social Sciences (SPSS) and then analysed to obtain frequencies, percentages, cross-tabulations, χ2 test, and odds ratios (OR). Considering a 95% confidence interval, a p-value less than 0.05 was considered statistically significant.
Results
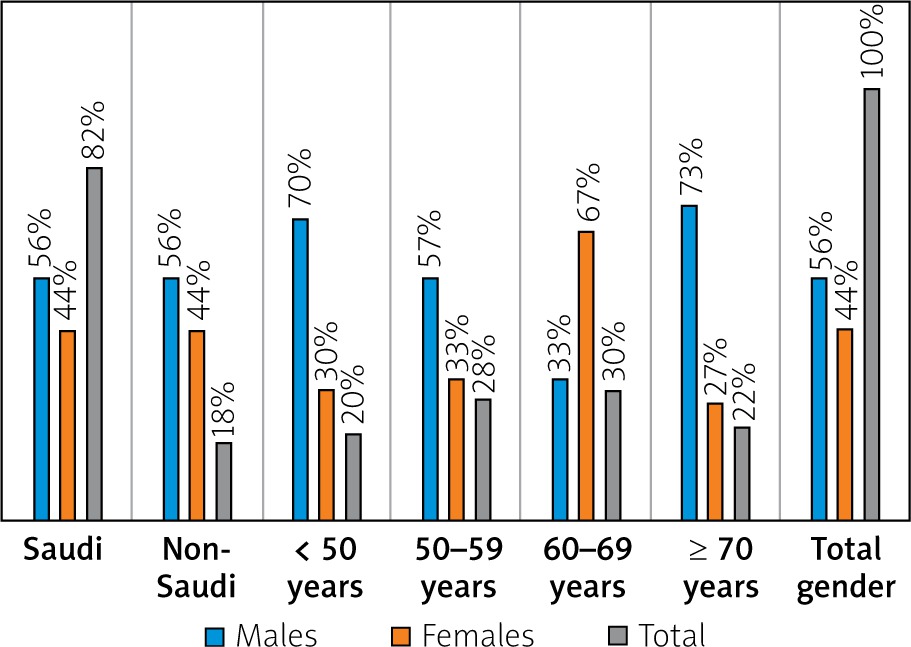
The 50 studied cases (41 (82%) Saudi and 9 (18%) non-Saudi) included 28 (56%) males and 22 (44%) females, aged 29 to 86 years with a mean age ± STD of 58.6 ±1.29 years. The male: female ratio was 1.27 : 1.00, as shown in Table I and Figure 1.
Table I
Distribution of patients by nationality, age, and gender
| Variable | Males | Females | Total | |
|---|---|---|---|---|
| Nationality: | ||||
| Saudi | 23 | 18 | 41 | |
| Non-Saudi | 5 | 4 | 9 | |
| Total | 28 | 22 | 50 | |
| Age group [years]: | ||||
| < 50 | 7 | 3 | 10 | |
| 50–59 | 8 | 6 | 14 | |
| 60–69 | 5 | 10 | 15 | |
| ≥ 70 | 8 | 3 | 11 | |
| Total | 28 | 22 | 50 | |
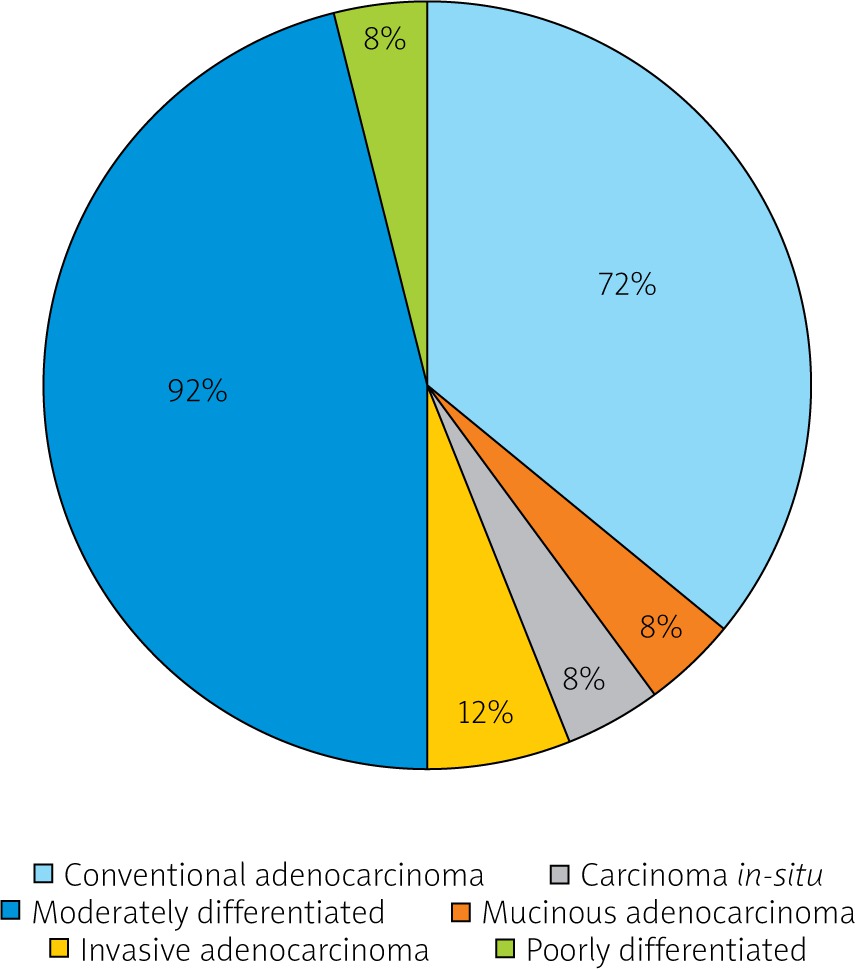
The diagnosed colon cancers included conventional adenocarcinoma 36 (72%), mucinous adenocarcinoma 4 (8%), carcinoma-in-situ 4 (8%), and invasive adenocarcinoma 6 (12%). Moderately differentiated and poorly differentiated stages were confirmed in 46 (92%) and 4 (8%), respectively, as shown in Figure 2.
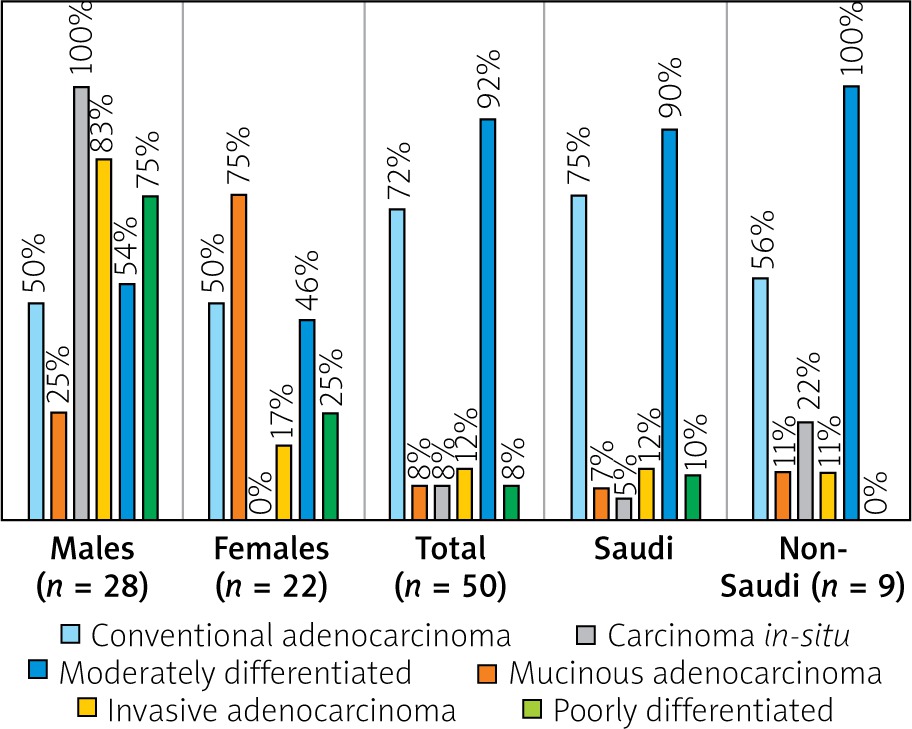
Conventional adenocarcinoma was presented equally in both sexes. Mucinous adenocarcinoma was more frequent among females 3 (75%), whereas carcinoma in situ 4 (100) and invasive adenocarcinoma 5 (83%) were more common among males. Males and females have a similar grade of presentation (moderately differentiated); hence, poorly differentiated grade was commonly seen in males 3 (75%), as indicated in Table II and Figure 3.
Table II
Distribution of the histopathological diagnosis by gender and nationality
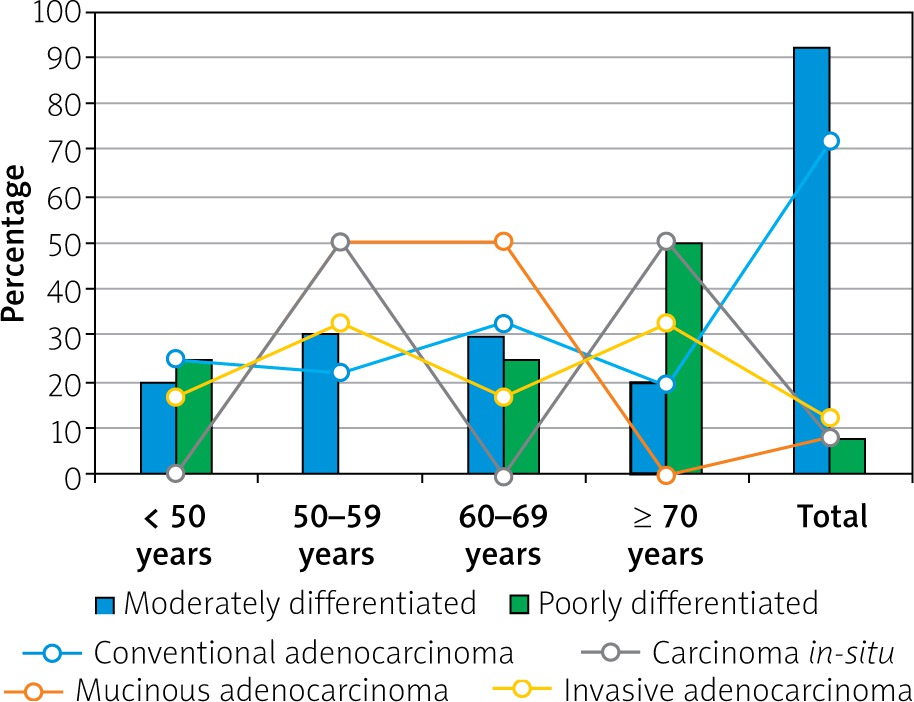
Most cases of conventional adenocarcinoma were found among age ranges 60–69 years followed by < 50 years, representing 12/36 (33%) and 9/36 (25%), respectively. All cases of mucinous adenocarcinoma were found in the range 50–69 years (4 (100%)). The cases with poorly differentiated carcinoma were frequently seen in the age range ≥ 70 years (3 (75%)), as indicated in Table III, Figures 4–6.
Table III
Distribution of the histopathological diagnosis by gender and age
Discussion
The present study’s findings indicate that many Saudi Arabian patients present with colon cancer at an early age with advanced stages of the disease, and men were more frequently affected than females. About 20% of the patients presented at age < 50 years, which is globally considered younger age [12], and most of them were males. However, several factors might contribute to the overall increased prevalence of this condition, such as lack of physical activity, dietary factors, and obesity; however, the increased prevalence among the younger generation may stimulate thinking about a better understanding of the genetic processes underlying the disease in this population. Such approaches may offer the opportunity of establishing evidence-based strategies for screening and clinical management for better outcomes in this section of the population [13]. Factors such as race and tumour biology have been suggested to contribute to the diversity of colon cancer in all ages [14, 15]. Moreover, it is well established that colon cancer is more frequent among males [14].
In the present study, all of the colon lesions were adenocarcinomas, with predominantly revealed conventional adenocarcinoma. This is in agreement with the available facts in the literature stating that the adenocarcinoma variant represents more than 90% of colorectal carcinomas [16]. However, a mucinous variant was identified in 8% of the cases in the present series. Mucinous adenocarcinoma of the colon represents a variant with worse survival outcomes than other variants [17]. This type of colon cancer is identified by a large amount of extracellular mucin (approximately 50% of the tumour bulk). Mucinous adenocarcinoma represents 10% to 20% of CRC. It is more frequently seen in younger females [18], which is supported by the findings of the present study’s findings (75% of the patients with mucinous adenocarcinoma were females, and about 50% were aged less than 60 years).
About 92% of the cases were categorized as moderately differentiated tumours, and the remaining 8% of patients were found to have poorly differentiated lesions. About 70% of colorectal adenocarcinoma are identified in moderately differentiated grades, whereas poorly differentiated represents 10% to 20% of the diagnosed CRC cases [19]. However, studies from Saudi Arabia have shown that more than 70% of cases of colorectal cancers are diagnosed at the late stages of the diseases, indicating the ineffectiveness of the screening and other control measures in the country [20, 21]. A study from North West Saudi Arabia has shown that most of the patients with CRC presented with intestinal obstruction, and there were more younger patients than older patients, and females were more frequent than males, which is in line with the findings of the present study [22]. These findings necessitate urgent intervention of national policies to detect small cancers and precancer by implementing sustainable screening programs to identify patients at risk. This will ultimately reduce the number of cases presenting with advanced stages of CRC in the country [23].
Althought the present study has some limitations, including its small sample size and its retrospective setting, it provides valuable information for health policymakers and health providers in the course of overall colorectal cancer management in Saudi Arabia. Moreover, the study clarified the areas for future research in environmental and genetic associated clues of colorectal cancer.
Conclusions
Conventional adenocarcinoma is the most common presenting colon cancer, and at a relatively young age. Mucinous adenocarcinoma frequently presents in female patients of a somewhat more youthful generation. Most patients are diagnosed with moderately differentiated adenocarcinoma, followed by poorly differentiated adenocarcinoma. The findings necessitate urgent intervention of national policies for early detection by implementing sustainable screening programs.










