









Introduction
Colorectal cancer (CRC) is regarded as the third most frequent malignant tumour worldwide, and its rate of mortality has increased over the past several decades due to recurrence and metastasis [1]. Despite advances in cancer treatments and management of CRC, prognostic biomarkers remain a promising way to predict the outcome of cancer [2]. Currently, some prognostic factors, such as tumour TNM stage, cell differentiation grade, and vascular invasion, have been widely utilised as the most accurate predictors of tumour recurrence and prognosis [3]. However, the survival outcome varies widely even in patients with the same TNM stage and tumour differentiation grade. Therefore, to estimate more specific oncological outcomes, novel prognostic markers are also required.
Strong evidence has confirmed that systemic inflammatory response is known to play a vital role in human cancer development and progression [4]. Tumors are closely related to inflammation. Inflammation is an essential component of the tumour microenvironment, and the changes in inflammatory cells might influence tumour progression, such as neoplastic cell proliferation, migration, invasion, collapse of anti-tumour immunity, metastasis, and so forth [5, 6]. Accumulating evidence shows that the peripheral neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) have been widely proposed as prognostic factors for many malignancies such as gastric cancer [7], nasopharyngeal carcinoma [8], liver cancer [9], and especially colorectal cancer [10]. Moreover, it is likely that the tumour microenvironment as well as systemic inflammatory response might be changed because of surgery [11]. However, only a few studies have assessed the relationship between dynamic changes of these perioperative inflammatory markers and survival prognosis in such patients.
Aim
In the present study, we hypothesised that both predictors are associated with prognostic survival in CRC patients who have undergone curative surgery. Furthermore, we compared perioperative changes to evaluate the prognostic significance of patients’ survival.
Material and methods
This study was conducted according to the Declaration of Helsinki and was approved by our Hospital. Written, informed consent was obtained from all individual participants included in the study.
Patient selection
A total of 183 CRC patients treated with curative surgery at the Department of Colorectal Surgery in our hospital from January 2007 to January 2013 were reviewed. Patients are excluded if they suffered from infection, haematological diseases, hyperpyrexia, renal dysfunction, diabetes mellitus, and other acute or chronic diseases, or if they had received previous chemotherapy, radiotherapy, or other targeted therapy. Postoperative follow-ups were generally performed by letter and by telephone interview every 3–6 months until death or 5 years and were ended after January 1, 2018.
Perioperative model of NLR and PLR
Preoperative blood samples were obtained prior to the surgical operation. The median interval between pre- and postoperative blood tests was 14 days. For the calculation of the NLR and PLR, NLR was defined as the absolute neutrophil count divided by the absolute lymphocyte count, and PLR was also conducted in the same way. The cut-off value for haematological profiles was determined using the receiver operating characteristic (ROC) curve analysis. According to the cut-off value, all patients were divided into four groups: HH, patients with both high preoperative and postoperative values; HL, patients with high preoperative and low postoperative values; LH, patients with low preoperative and high postoperative values; and LL, both low preoperative and postoperative values. Medical records were assimilated with respect to the patients’ age, sex, and clinicopathological characteristics (such as location, size, histological type, TNM stage, invasion, and lymph node).
Statistical analysis
The end points of this study were recurrence-free survival (RFS), which was defined as the time from the first day of palliative operation to the disease progression or recurrence, and overall survival (OS), which was defined as the time from the first day of palliative operation to death by any cause or to the last follow-up. ROC analysis determined the optimal cut-off value as a predictive marker for OS and RFS. The association between the clinicopathological characteristics and perioperative change of the four groups were compared using the χ2 test or Fisher’s exact probability test. The survival curves were generated using the Kaplan-Meier method, and the differences were compared using the log-rank test. The univariate analysis assessed the prognostic factors, and multivariate analysis (Cox’s proportional-hazards regression model) evaluated the independent factors for survival prognosis. P-values < 0.05 were considered statistically significant. The statistical analysis was performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient demographics and clinicopathological characteristics
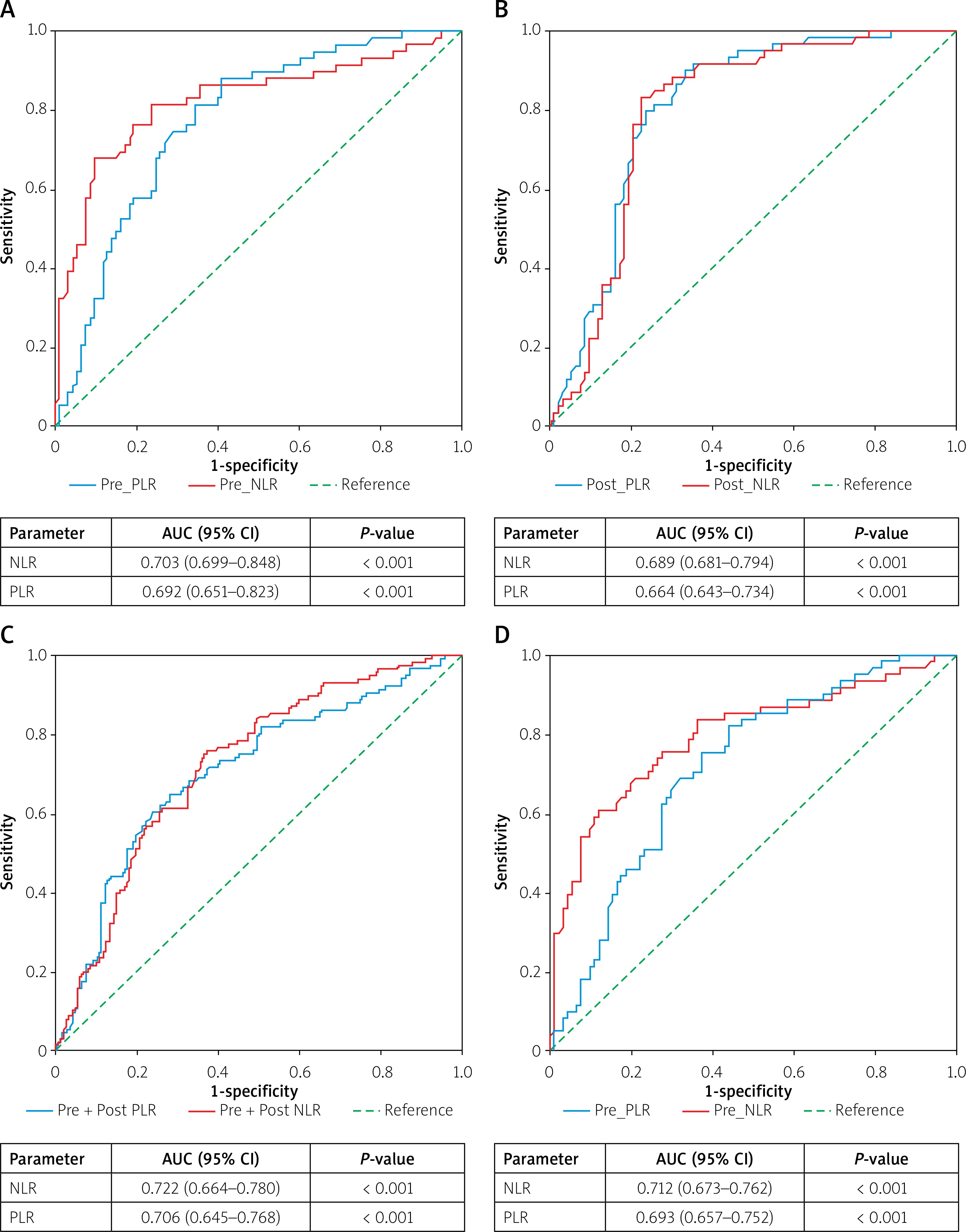
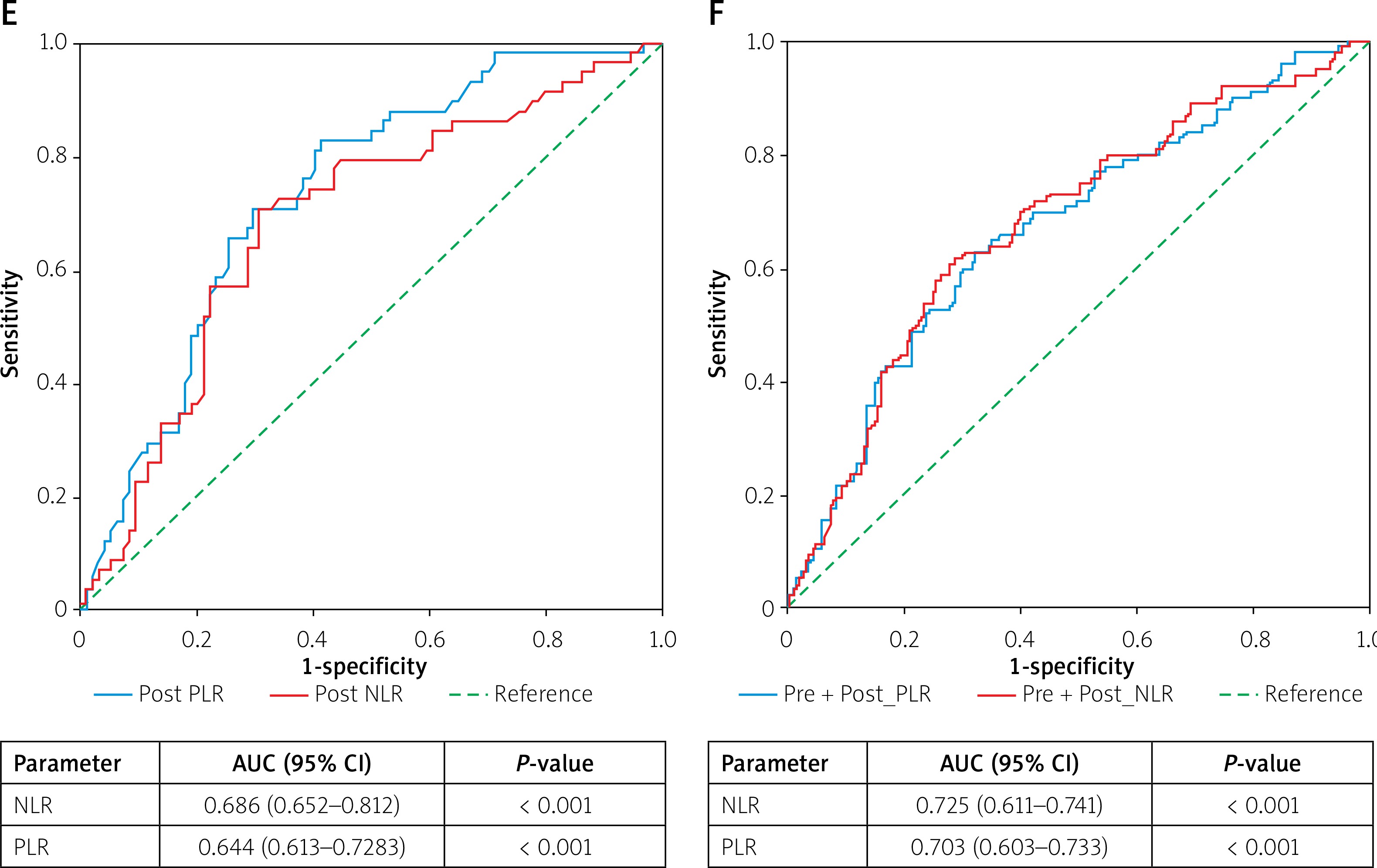
Table I shows the clinicopathological characteristics of the 183 patients in the study. The female-to-male ratio was 85:98, and the median age was 69 years, ranging from 45 to 79 years. Patients predominantly suffered from rectal cancer (64.48%), and 58.47% of patients presented tumour size ≥ 3 cm. The clinical TNM stage revealed the pathological diagnoses as follows: 37 patients with stage I, 67 patients with stage II, 49 patients with stage III, and 30 patients with stage IV. Moreover, the histological grade revealed 121 patients in G1-2 and 62 patients in G3-4. In terms of cancer invasion, high grades (T1-2) constituted 94 patients, and the other grades (T3-4) constituted 99 patients. A total of 71 patients presented lymph node with negative tumour (N0), while 112 patients were positive, and 109 patients received postoperative adjuvant chemotherapy. ROC analysis could calculate the sensitivity and specificity levels of NLR and PLR as survival estimation predictors, as shown in Figure 1. For RFS, pre- and post- NLR showed a larger AUC than pre- or post- NLR. Moreover, the predictor of PLR showed similar results. Regarding OS, pre- and post-NLR/PLR was superior to the pre- or post-NLR/PLR. The optimal cut-off values of perioperative NLR and PLR were pre-2.94, post-4.32 and pre-184.29, post-212.37, respectively. Furthermore, we divided the patients into four groups according to these perioperative cut-off values. Table I also shows the distribution of patients in these four groups. Patients with higher cancer stage, poorer differentiation, and greater lymph node metastasis were significantly associated with perioperative NLR or PLR (all p < 0.05). Conversely, no difference was observed in age, gender, tumour location, size, and adjuvant chemotherapy (all p > 0.05).
Table I
Comparison between groups stratified by perioperative changes and patients’ clinicopathological
Comparison between survival prognosis and perioperative changes
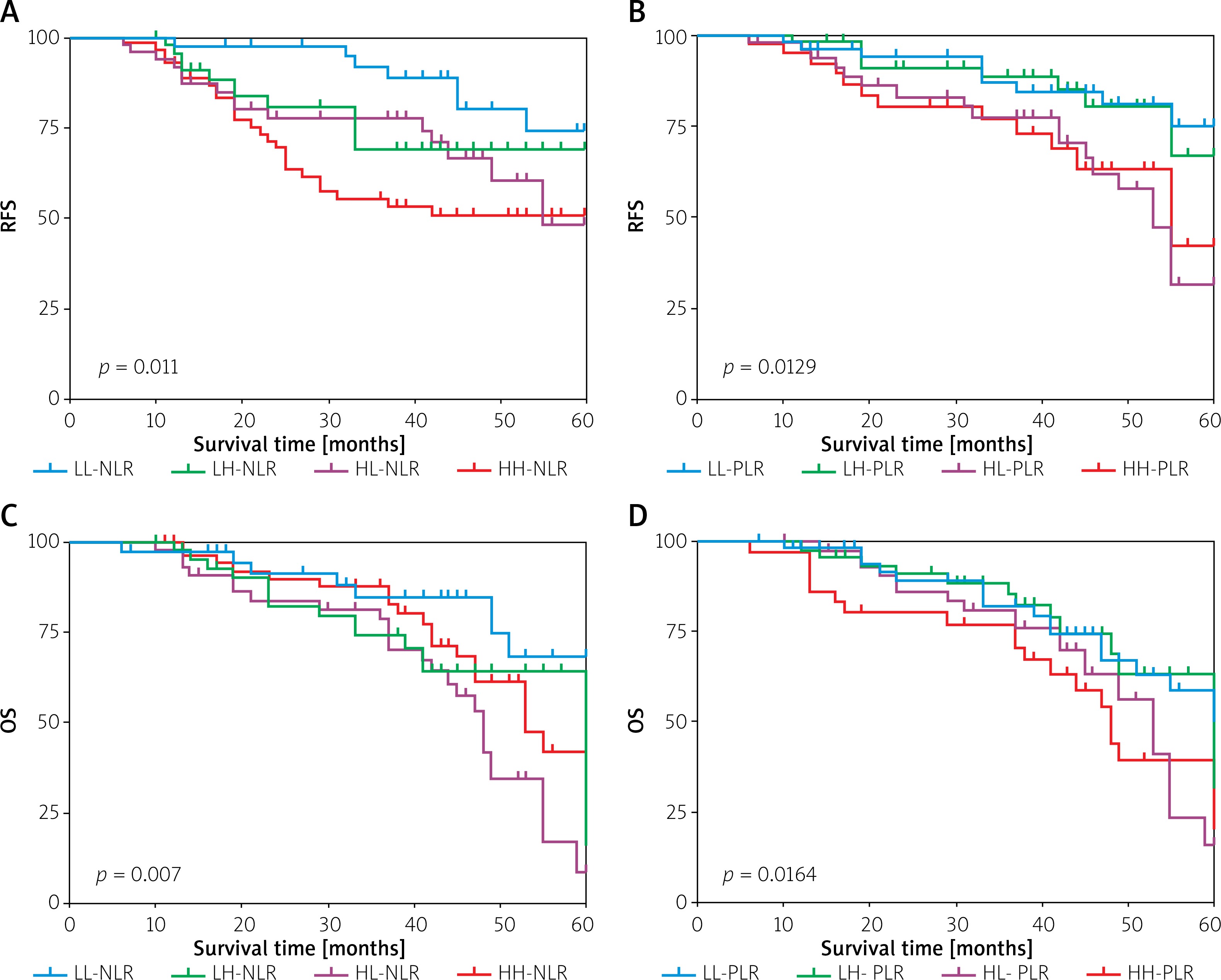
According to the follow-up period, 61 (33.33%) patients had recurrence: 22 patients presented local recurrence and 39 patients developed distant metastasis. Seventy-six (41.53%) patients died: 33 patients from tumour recurrence, one from chemotherapeutic toxicity, and the other patients due to unknown reasons. For prognosis of patients according to the Kaplan-Meier curve and log-rank test, the four groups (LL, LH, HL, and HH) stratified by perioperative changes had significantly different RFS and OS, as shown in Figure 2 (all p < 0.05). Thus, perioperative changes of NLR and PLR could effectively predict the prognostic survival of CRC patients in the present study.
Prognostic variables for RFS and OS
With respect to all prognostic factors, Tables II and III showed the results of univariate and multivariate analysis of various parameters in terms of RFS and OS. Univariate analysis revealed that patients with high cancer stage, poorer differentiation grade, severer invasion and lymph node metastasis, no adjuvant chemotherapy, and greater perioperative change of NLR/PLR (HH, LH) were obviously associated with worse RFS and OS (all p < 0.05). Although tumour location was significantly associated with poor OS (p < 0.05), it was not related to RFS. Factors with p < 0.05 in univariate analysis were conducted for further multivariate analysis. Patients with higher cancer stage, lymph node metastasis, and perioperative change of NLR/PLR (HH, LH) had significant association with poor prognosis of OS and RFS (all p < 0.05). Simultaneously, it suggested that LH-NLR/PLR is a protective factor for survival (HR < 1).
Table II
Univariate and multivariate analysis of factors associated with recurrence-free survival
Table III
Univariate and multivariate analysis of factors associated with overall survival
Discussion
To our knowledge, this is the first study to evaluate the associations between perioperative changes of NLR and PLR and the postoperative outcome in patients with CRC, who underwent palliative resection of the primary tumour. Our results indicate that perioperative changes of NLR and PLR as biomarkers to predict prognosis would help to elucidate the survival rates in such patients.
Various studies have indicated that changes in immune cellular components in peripheral venous blood could reflect the inflammation status of the tumour, which is valuable in predicting survival prognosis [12, 13]. It is increasingly speculated that the inflammation and tumour are correlated, resulting in the establishment of novel biomarkers of cancer for the evaluation of the prognostic significance [14]. Reportedly, neutrophils reflect the status of the systematic inflammation and accelerate the remodelling of the extracellular matrix [15]. This, in turn, stimulates the tumour-cell proliferation, migration, and metastasis via the enzymatic actions, such as the release of reactive oxygen species (ROS), nitric oxide (NO), and anginas [16]. Moreover, neutrophilia activates the inflammatory response to promote the tumour growth by pro-angiogenic and growth factors [17]. Another study showed the lymphocyte infiltration response to the tumour. Increased lymphocytic reactions have been associated with a better outcome [18]. In addition, platelets could secrete cellular growth factors such as platelet-derived growth factor, vascular endothelial growth factor, transforming growth factor β, and platelet factor 4, followed by the stimulation of tumour angiogenesis and growth [19, 20]. Therefore, NLR and PLR represent the tumour-inflammatory response, which indicates the degree of tumour progression and contributes to the prediction of survival prognosis.
However, there is a great deal of risk and bias in using only one index for detection. For more comprehensive assessment of prognosis in this study, we use the combined preoperative and post-operative changes of both biomarkers to increase the predictive accuracy for survival compared with preoperative or postoperative ones alone. ROC analysis indicated that pre- and post-NLR/PLR were superior to the pre- or post-NLR/PLR for RFS and OS, respectively. The change of tumour status and surgical stress may affect systemic inflammation as well as oncological outcome [21]. It is conceivable that significant tumour reduction after surgery may lead to improvement of systemic inflammation as well as immunological response [22]. It is reported that the surgery itself promotes the release of tumour emboli and induces immunosuppression that favours the survival and progression of cancer [23]. We also found that the change in perioperative NLR/PLR was independently associated with elevated risk for RFS and OS. Simultaneously, it indicated that LH-NLR/PLR seems to be a protective factor for survival (HR < 1). Although this stratification requires external validation, it may enable us to identify patients with risk or protective factors.
Besides perioperative NLR/PLR factors, cancer stage, lymph node, and adjuvant chemotherapy were also identified as robust prognostic indicators in the univariate and multivariate analysis, which is consistent with the results of previous studies [24, 25]. However, our study showed that tumour invasion and cancer grade were associated with poor prognosis in the univariate analysis but not in the multivariate analysis. Compared with previous prognostic indicators, this inflammatory biomarker has the advantage of being simple, easily available, economical, objective, and reproducible, and it could be measured at the beginning of chemotherapy treatment and monitored throughout the entire therapy period [26].
Nevertheless, our study has some limitations that should be mentioned. First, it is a retrospective investigation; thus, a potential bias in the selection of patients is inevitable. Second, surgery was performed by several surgeons, which possibly influenced oncological outcome. Finally, the current study lacked any evaluation of tumour-associated neutrophils and lymphocytes, which could cause different immune responses.
Conclusions
The current study suggests that perioperative NLR/PLR might be a good predictor for prognosis in CRC patients undergoing curative surgery. It is recommended as a practical tool to assess the prognosis of RFS and OS. Thus, these findings provided an in-depth understanding of the patients, which could help guide a customised therapeutic strategy.