
Introduction
Irritable bowel syndrome (IBS) has emerged as an important medical problem with a major impact on global health care systems and patients’ quality of life. IBS lies in the spectrum of functional gastrointestinal disorders (FGIDs), recently named disorders of gut-brain interaction (DGBIs). According to Rome IV criteria, FGIDs/DGBIs are classified by gastrointestinal symptoms related to a combination of any of the following: i) motility disturbances, ii) visceral hypersensitivity, iii) altered mucosal and immune function, iv) gut microbiome, and/or v) central nervous system functioning [1, 2]. For the 2 most common DGBIs syndromes – IBS and functional dyspepsia (FD) – the worldwide prevalence ranges from 1.1% to 57%, which could reflect the scale of methodological heterogeneity, differences among surveyed populations, or methodological biases among reported studies [3]. Several factors could contribute to various biases of outcomes in IBS studies, including (yes or no) reporting of the following: i) comorbid conditions, ii) dietary habits, iii) mental health status, iv) ethnicity, v) timing of enrolment, vi) recording of menses, vii) the use of a run-in periods, viii) effect size and formal statistical power analysis, ix) clinical endpoints, x) fluctuations in symptoms, and xi) the potential for wide variations in bowel habits [4]. In the most recent large-scale multinational study, comprising 33 countries, the investigators reported that more than 40% of persons worldwide suffer from FGIDs/DGBIs with IBS rates between 3% and 5% in most countries [3].
The treatment of IBS consists of various pharmacological and non-pharmacological modalities; however, the data of long-term follow-up for most of them are scarce [5, 6]. Many patients initially benefit from placebo effect [7, 8] but respond poorly to longer-term treatments [9], either do not tolerate or not respond to pharmacotherapy, and may be worried by potential adverse events [10]. Finally, some patients may become dissatisfied with doctors’ advice and treatment options. Modulation of gastrointestinal microbiota by means of probiotics and prebiotics is often sought, advertised as a popular treatment modality among IBS patients [11]. Faecal microbiota transplantation (FMT) currently is not routinely recommended for IBS treatment and requires further methodological assessments [12].
To date, experts, authorities, and medical societies conduct and aim to publish well-powered, appropriately-designed studies and offer their interpretation of data with a high level of evidence (i.e. systematic reviews and meta-analyses) to draw conclusions or develop guidelines and recommendations. Until now numerous guidelines and recommendations have been published concerning the role of probiotics in IBS. Of note, claims for probiotics in foods in the European Union (EU) are yet to be granted by the European Food and Safety Authority (EFSA). Therefore, medical experts still recommend probiotics on the basis of scientific literature and recommendations preferably released by independent and non-commercial health authorities.
In the last decade numerous guidelines and recommendations evaluating the utility of probiotics in IBS have been published [13–16]. However, not all reports available on the Internet are adhering to standards of evidence-based medicine (EBM), lacking scientific validity, and presenting contrasting conclusions, which makes clinical judgment difficult. Sadly, uncertainty among medical professionals regarding the choice of probiotics in IBS still exists. Similarly, patients’ queries to medical practitioners regarding the role of probiotics in their digestive misalignments, including IBS symptoms, are frequent. The questions raised are often difficult to answer because most of the probiotics available on the market are registered as food supplements, frequently with no clear evidence of efficacy.
Aim
Therefore, we aimed to analyse published recommendations and guidelines regarding the clinical effectiveness of various probiotic strains recommended to adults with IBS.
Material and methods
The strategy to evaluate the papers relevant to our aims comprised the following steps: 1) searching for relevant recommendations/guidelines, 2) applying exclusion criteria, and 3) synthesizing guideline recommendations to identify issues potentially relevant to the efficacy of probiotics in IBS.
Data Sources and Search Terms
For the present rapid review, we conducted a search in PubMed/Embase/Google Scholar up to 15 May 2021, using the following search terms:
Embase: (‘irritable bowel syndrome’ OR ibs OR ‘digestive system function disorder’/exp OR ‘digestive system function disorder’ OR ‘functional gastrointestinal disorder’ OR ‘gastrointestinal dysfunction’ OR ‘gastrointestinal function disorder’ OR ‘gastrointestinal tract function disorder’) AND ‘treatment’ OR ‘management’ OR ‘drugs’ OR ‘agents’ OR ‘therapy’ OR ‘clinical practice’ OR ‘probiotic agent’/exp OR ‘probiotic’ OR ‘probiotic agent’ OR ‘probiotics’ OR ‘synbiotic agent’/exp OR ‘synbiotic’ OR ‘synbiotic agent’ OR ‘synbiotics’ OR ‘microbes’ OR ‘beneficial microbes’ OR ‘beneficial bacteria’) AND (‘systematic review’/exp OR ‘review, systematic’ OR ‘systematic review’ OR ‘practice guideline’/exp OR ‘recommendations’/exp).
PubMed: (irritable bowel syndrome OR ibs OR digestive system function disorder OR digestive system function disorder OR functional gastrointestinal disorder OR gastrointestinal dysfunction OR gastrointestinal function disorder OR gastrointestinal tract functiondisorder) AND (treatment OR management OR drugs OR agents OR therapy OR clinical practice OR probiotic OR probiotic agent ORprobiotics OR synbiotic agent OR synbiotic OR synbiotic agent OR synbiotics OR microbes OR beneficial microbes OR beneficial bacteria) AND (systematic review OR review, systematic OR systematic review OR practice guideline OR recommendations).
The electronic search was supplemented by a manual review of the reference lists from eligible publications and relevant reviews. Taking into account recently published guidelines exploring the role of probiotics in IBS by major gastrointestinal societies, the most recent being from the American Gastroenterology Association (AGA) [17, 18] and the British Society of Gastroenterology (BSG) [19], we decided to present to outcomes of our analysis in the form of a rapid review and synthesis of data, in which parts of the systematic review process are either simplified or omitted to obtain the information in a timely manner. Because our study is a rapid review the results are potentially not exhaustive. The eligible papers were chosen by 2 authors (PK and WM).
Inclusion and exclusion criteria
Our inclusion criteria were as follows:
documents (recommendations/guidelines) in which the effectiveness of probiotics in patients with IBS was analysed;
documents (recommendations/guidelines) in adult humans (> 18 years old);
documents in English, German, and Polish;
recommendations/recommendations of scientific societies, medical organizations, and expert groups that are formalized.
Exclusion criteria were:
Outcomes
After selecting the papers, we abstracted data on the following sections: i. general statement of the authorities, ii. level of recommendation along with the quality of evidence, and iii. recommended probiotic strains. The Excel files with abstracted data completed by each investigator were compared with the content of the others’ files, and any discrepancies were solved by the last author by consensus.
Pooling results
We conducted a random effects [20] meta-analysis of outcomes for which ≥ 2 studies contributed data on the same probiotic strain, using Comprehensive Meta-Analysis V3 (http://www.meta-analysis.com). We explored study heterogeneity using the χ2 test of homogeneity, with p < 0.05 indicating significant heterogeneity. All analyses were 2-tailed with alpha equal to 0.05. Categorical outcomes (global symptoms and abdominal pain persistence) were analysed by calculating the pooled risk ratio (RR). We inspected funnel plots and used Egger’s regression test [21] and the Duval and Tweedie’s trim and fill method [22] to quantify whether publication bias could have influenced the results.
Results and discussion
We identified 17 papers presenting guidelines or recommendations for probiotics in irritable bowel syndrome. Overall, in 13 guidelines/recommendations, probiotics were recommended, whilst in 4 statements no recommendation or “advise to use probiotics only in the content of clinical trial” were given. The position statements of societies’ recommendations regarding the use of probiotic strains in IBS are presented in Table I (synthesis of the recommendations related to probiotic therapy in IBS). The dose and duration of probiotic therapy reported across IBS guidelines are presented in Table II. The quality of evidence among selected guidelines and recommendations varied from very low to moderate. The level of recommendation ranged from no recommendation (AGA 2021) [17, 18], through conditional (CAG 2019) [16], to strong recommendation (JSGE 2021) [14]. Most of the reports followed systematic methods to search for evidence. Moreover, a diverse multidisciplinary working group of clinicians and academics with experience in primary, secondary, or tertiary care, as well as dietetics, were involved in some more recent guidelines [17] working with the collaboration of IBS patient networks, using the Grading of Recommendations Assessment, Development, and Evaluation system to evaluate the strength of the recommendations and the overall quality of evidence [17]. However, the majority of positive recommendations for probiotics in IBS declared insufficient evidence for any particular probiotic strains or species.
Table I
Summary of existing guidelines and recommendations on probiotic strains in irritable bowel syndrome
| Organisation/country/year | Summary of statement | Recommendation level | Quality of evidence | Recommended strains |
|---|---|---|---|---|
| German Society for Digestive and Metabolic Diseases (DGVS, Deutsche Gesellschaft für Verdauungs- und Stoffwechselkrankheiten) German Society for Neurogastroenterology and Motility (DGNM, Deutsche Gesellschaft für Neurogastroenterologie & Motilität In collaboration with other German medical societies* [39] | Probiotics recommended in most/some IBS patients with pain and diarrhoea, constipation and bloating/abdominal distension/meteorism/flatulence Bifidobacterium infantis 35624 Bifidobacterium animalis ssp . lactis DN-173 010 Lactobacillus casei Shirota Lactobacillus plantarum 299v Lactobacillus rhamnosus GG (only in children) E. coli Nissle 1917 | Recommendation strength Evidence level A Meaning for physicians: different decisions are appropriate for different patients, depending on the patient’s situation but also on personal opinions and preferences Meaning for patients: The majority of patients (> 50%) would decide in favour of the intervention, but many would not | Strong consensus | Data for individual strains are shown in Table II |
| Experts of Yale Workshop on Probiotics/USA/ 2011, 2015 [40, 41] | Only the following strains are recommended in text: Bifidobacterium infantis B5624, VSL#3 Bifidobacterium animalis Lactobacillus plantarum 299V | ND | Recommendation is based on positive-controlled studies, but the presence of some negative studies that did not support the primary outcome. Recommendation is based on some positive studies, but clearly inadequate amount of work to establish certainty | Data for individual strains are shown in Table II |
| British Dietetic Association (BDA)/UK/2012 [13] | Probiotics can be considered secondary to other second-line advanced dietary interventions. If one probiotic does not improve symptoms, they could trial a different product. Awareness: 1) Some products contain ingredients that may increase IBS symptoms (fructans, polyols, fructose and lactose) 2) If a probiotic is found to be beneficial after 4 weeks of use, it can be continued, although the long-term effects are not known 3) Once a probiotic is stopped, the bacterial strain(s) will gradually cease to colonise the gut or reduce in numbers | ND | Limited weak | There is insufficient good evidence to recommend a specific product, however one strain and one multistrain product were listed. Data for individual strains are shown in Table II |
| American College of Gastroenterology (ACG) – monograph on IBS/USA/2014 [17, 42] | Probiotics improve global symptoms, bloating, and flatulence in IBS | Weak | Low | Recommendations regarding individual species, preparations, or strains cannot be made at this time because of insufficient and conflicting data |
| British Dietetic Association (BDA)/UK/2016 [13] | Probiotics are unlikely to provide substantial benefit to IBS symptoms. However, individuals choosing to try probiotics are advised to select one product at a time and monitor the effects. They should try it for a minimum of 4 weeks at the dose recommended by the manufacturer. Taking a probiotic product is considered safe in IBS | ND | Grade B (not explained in text) | No strain specific recommendation was made; however, 18 evidence statements were developed demonstrating clinically useful efficacy for dose-specific probiotics, and one further evidence statement lists 12 dose specific probiotics found to be ineffective. Data for individual strains are shown in Table II |
| World Gastroenterology Organisation (WGO)/Global Guidelines/2017 [43] | A reduction in abdominal bloating and flatulence as a result of probiotic treatments is a consistent finding in published studies; some strains may ameliorate pain and provide global relief. The literature suggests that certain probiotics may alleviate symptoms and improve the quality of life in patients with functional abdominal pain | ND | ND | Data for individual strains are shown in Table II |
| Korean Society of Neurogastroenterology and Motility (KSNM)/Korea/ 2018 [44] | Probiotics may be considered to relieve global symptoms, bloating, and flatulence in irritable bowel syndrome patients | Weak: The best action may differ depending on the circumstances or patient or society values. Other alternatives may be equally reasonable. The desired effect may be slightly greater than the harmful effect | Low quality: Further research is very likely to have an important impact on our confidence in the prediction of the effects and is likely to change the prediction. Evidence for at least one critical outcome from observational studies, case series, or RCTs with serious flaws; indirect evidence; or a consensus among experts | The optimal strains, species, or combinations thereof, and the appropriate dose and duration, are unclear |
| Experts’ opinions: completely agree (7.5%), mostly agree (55.0%), partially agree (27.5%), mostly disagree (7.5%), completely disagree (0.0%), and not sure (2.5%) | ||||
| Polish Society of Gastroenterology/Poland/ 2018 [45] | We suggest using certain strains or a combination of probiotic strains tested for their efficacy in IBS, rather than probiotics as a group, to reduce overall symptoms of IBS as well as bloating and diarrhoea in patients with IBS. The probiotics with expected beneficial effects in patients with IBS and known levels of bacteria per dose are listed in Table II It is not possible to determine the efficacy of individual strains included in combined preparations or the efficacy of other configurations (blends) of the aforementioned strains | Weak Weak Weak | Very low Moderate Very low | Data for individual strains are shown in Table II |
| Vote Full acceptance – 57.1%; Acceptance with certain reservations – 28.6%; Acceptance with serious reservations – 14.3%; Rejection with certain reservations – 0%; Full rejection – 0%. Agreement level: high | ||||
| American College of Gastroenterology (ACG) – Monograph on Management of IBS/USA/ 2018 [46] | Probiotics, taken as a group, are suggested to improve global symptoms, as well as bloating and flatulence in IBS patients | Weak | Weak | No strain was recommended |
| South East Asian Gastro-neuro Motility Association (SEAGMA)/Asia/2018 [41] | Probiotics have beneficial effects in irritable bowel syndrome | There is good evidence to support the statement | Evidence obtained from at least 1 RCT | No strain was recommended |
| Voting: Accept completely 5.88%; Accept with some reservation 47.06%; Accept with major reservation 23.53%; Reject with reservation 23.53%; Reject completely 0% | ||||
| Canadian Association of Gastroenterology/Canada/2019 [16] | We suggest offering IBS patients probiotics to improve IBS symptoms | Conditional recommendation | Low-quality evidence | Insufficient evidence for any particular species. Limited therapeutic trial (e.g., one month) is suggested |
| Vote: strongly agree, 25%; agree, 67%; neutral, 8% | ||||
| The Asian Neurogastroenterology and Motility Association (ANMA) – Second Asian Consensus/Asia/2019 [15] | The effectiveness of probiotics has not been fully validated in IBS | No recommendations | Moderate | No strain was recommended |
| Level of agreement: accept completely – 85.7%, accept with minor reservation –4.8%, accept with major reservation – 9.5%, reject with major reservation – 0%, reject with minor reservation - 0%, and reject completely – 0% | ||||
| American Gastroenterological Association (AGA)/USA/2020. [17, 42] | The use of probiotics is recommended only in the context of a clinical trial | No recommendations | Very low | No strain was recommended |
| Knowledge gap | ||||
| American College of Gastroenterology (ACG) Clinical Guideline: Management of IBS/USA/2021 [47] | We suggest against probiotics for the treatment of global IBS symptoms | Conditional recommendation | Very low level of evidence | No strain was recommended |
| Japanese Society of Gastroenterology (JSGE)/Japan/2021 [14] | Probiotics are effective in treating IBS. Probiotics are recommended for IBS. Combination therapy with probiotics and Mosapride was effective for the relief of symptoms | Strong | High | Lack of comments concerning special strains |
| 100% agreed | ||||
| Romanian Society of Neurogastroenterology/Romania/ 2021 [48] | In patients with IBS, the use of probiotics as an alternative therapy is recommended in trials of limited duration | Weak | B - Several studies available, at least one of high quality, others with limitations; trustworthy | No strain was recommended, further studies are warranted to establish strains efficiency, formulations, dosage, and treatment duration. Potential side effects awareness is needed |
| British Society of Gastroenterology/UK/2021 [19] | Probiotics can be an effective treatment for general symptoms and abdominal pain in IBS. However, it is impossible to recommend a specific species or strain. Patients wishing to try probiotics should take them for up to 12 weeks. When there is no improvement in symptoms, patients should stop taking them | Weak | Very low | No strain was recommended |
* German Society for Internal Medicine (DGIM, Deutsche Gesellschaft für Innere Medizin), Association of German Gastroenterologists in Private Practice (bng, Berufsverband Niedergelassener Gastroenterologen), Society for Paediatric Gastroenterology and Nutrition (GPGE, Gesellschaft für Pädiatrische Gastroenterologie und Ernährung), German Society for Nutritional Medicine (DGEM, Deutsche Gesellschaft für Ernährungsmedizin), German Society for General and Visceral Surgery (DGAV, Deutsche Gesellschaft für Allgemein- und Viszeralchirurgie), German College of General Practitioners and Family Physicians (Deutsche Gesellschaft für Allgemein- und Familienmedizin), German Society for the Study of Pain (DGSS, Deutsche Gesellschaft zum Studium des Schmerzes), German Society for Behavioural Medicine and Behaviour Modification (DGVM, Deutsche Gesellschaft für Verhaltensmedizin und Verhaltensmodifikation), German Society of Psychosomatic Medicine and Medical Psychotherapy (DGPM, Deutsche Gesellschaft für Psychosomatische Medizin und Ärztliche Psychotherapie), German Society for Tropical Medicine and International Health (DTG, Deutsche Gesellschaft für Tropenmedizin und Internationale Gesundheit), German Society for Naturopathy (Deutsche Gesellschaft für Naturheilkunde), German Irritable Bowel Self-Help (Deutsche Reizdarmselbsthilfe e. V.) (patient organization).
Table II
The most recent guidelines of the British Society of Gastroenterology (BSG) recommended dietary advice as a first-line strategy in all patients with IBS (recommendation: strong, quality of evidence: weak) and probiotics, as a group, as an effective treatment for global symptoms and abdominal pain in IBS (recommendation: weak, quality of evidence: very low) [19].
The study published recently by the American Gastroenterological Association (AGA) presented contrasting guidelines (no recommendations for probiotics in IBS due to insufficient data and knowledge gap) utilizing a process for developing clinical practice guidelines following the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach and best practices as outlined by the National Academy of Science (formerly the Institute of Medicine) [17]. In their recent guideline summary the AGA states: “Although there has been a substantial number of studies examining probiotics in various gastrointestinal diseases, the studies have been extremely varied, including differences in the strain of microbes used, dose, and route of administration, as well as the research methodology, including differences in the reporting of end points and outcomes. Furthermore, most of the studies with probiotics involved a relatively small number of patients compared to trials investigating the effects of pharmacological interventions. Conclusions drawn from meta-analyses or systematic reviews can be misleading if different studies with different patient populations, different reported end points and outcomes, or different strains or combinations of probiotics are grouped together inappropriately” [17].
Of all the analysed statements and recommendations, we paid attention to the most recent BSG guidelines on the management of IBS [19], which followed those recently released by AGA [17]. In contrast to the AGA recommendations, the BSG state that probiotics, as a group, may be an effective treatment for global symptoms and abdominal pain in IBS. Subgroup analyses of 45 randomized clinical trials (RCTs), randomizing 6352 patients according to type of probiotic used, demonstrated the strongest effects on global symptoms or abdominal pain for Lactobacillus (relative risk (RR) = 0.75; 95% confidence interval (CI): 0.60–0.94). However, variations in study design, strain, and species of probiotic used, and heterogeneity between studies did not allow for specific strain recommendations. Probiotic effects are strain dependent and should be documented in at least one RCT, preferably accompanied by confirmatory trials [23, 24]. Despite an overall large number of RCTs in IBS, only a few of them used the same probiotic strain. Therefore, we conducted subgroup analysis on Lactobacillus plantarum 299v (Lp299v) in comparison to other Lactobacilli reported in the most recent guidelines [19]. For 11 meta-analysed studies including 843 patients and investigating the effect of Lactobacillus species for global symptoms and abdominal pain in IBS, 82% heterogeneity (I2) was reported. Among them, 3 RCTs including 240 patients investigated the effect of Lp299v, reporting RR = 0.67 (p = 0.04) with I2 = 62.5 (p = 0.07). For other Lactobacilli, RR 0.79 (p = 0.08) with I2 = 80.3 (p < 0.001) were found. Publication bias for all Lactobacilli studies was not relevant (p = 0.59). A similarly low and statistically non-relevant I2 (51%, p = 0.09) was reported for IBS studies investigating the effect of Bifidobacteria, with 2 studies using the same probiotic strain Bifidobacterium bifidium HI-MIMBb75, but with overall less risk reduction (RR = 0.80; 95% CI: 0.70–0.91). In the case of Saccharomyces, 3 studies were meta-analysed with very high heterogeneity (I2 = 96%) and no significant effect on IBS global symptoms or abdominal pain (p = 0.18). Our current subgroup analysis (Figures 1 A, B) is in line with previous meta-analysis [25] reporting significant effects of Lp299v in reducing the risk of symptom persistence. Moreover this meta-analysis shows that a total favourable effect of Lactobacilli in IBS is driven by Lp299v. These observations “should considerably assist clinicians in making recommendations regarding the choice of probiotic that a patient should take” [26]. Of relevance are studies investigating the effects of probiotics in IBS in real-life settings. Of those reported in real life Lp299v significantly alleviated the global IBS symptoms, achieving maximum effect within 12 weeks of treatment [27], which is in line with the most recent guidelines as for time of probiotics administration [1]. These effects could be facilitated through unique mechanisms already known and described [28–32] for the Lp299v strain (Figure 2). Of importance, Lp299v fulfils the regulatory statements of Binda et al., which are as follows: “Probiotic strains must be (i) sufficiently characterized; (ii) safe for the intended use; (iii) supported by at least one positive human clinical trial conducted according to generally accepted scientific standards or as per recommendations and provisions of local/national authorities when applicable; and (iv) alive in the product at an efficacious dose throughout shelf life” [24]. Although the non-viable B. bifidum HI-MIMBb75 strain, also evaluated by Vasant et al. [19] in BSG recommendations, substantially alleviated IBS and its symptoms in real-life, according to the International Scientific Association for Probiotics and Prebiotics (ISAPP), dead microbes should not come under the probiotic classification [8]. As stated in current BSG guidelines [19], adverse event rates were similar in the probiotic and placebo arms, which is in agreement with the Agency for Healthcare Research and Quality (AHRQ), which reported no increased RR of the overall number of experienced adverse events (RR = 1.00; 95% CI: 0.93–1.07; p = 0.999), gastrointestinal, infections, and other adverse events, including serious adverse events (RR = 1.06; 95% CI: 0.97–1.16; p = 0.201), associated with probiotic intake [33]. This is important because consumer awareness on probiotics is rising, as is their intake for general digestive or health reasons [34]. Therefore, as well as guidelines, quality manufacturing control is critical for probiotic safety and efficacy. According to the FAO/WHO, probiotics are “live microorganisms which when administered in adequate amounts confer a health benefit on the host” [35]. All constituents of this definition should be taken into consideration when defining probiotic manufacturing and quality requirements. Most probiotics available on the market contain Lactobacilli or Bifidobacteria, as well as few other types of microorganisms. The choice of probiotic strains in the final probiotic product is based on biological, technological, and legislative factors. Probiotics undergo several technological and industrial steps, which include lyophilization (freeze-drying), with the potential to seriously alter their viability and end-product stability. Once ingested, probiotics initiate numerous physiological effects in the gastrointestinal tract (e.g. biofilm formation, release of bioactive substances, competing with other microorganisms). The evaluation of an effective probiotic dose is experimental. According to available literature the daily dose of ingested probiotic bacteria should range between 108 and 1011 CFU/day live bacteria [36]. The declared number of viable bacteria in the product should be maintained through the shelf-life date. Because the probiotic-related health properties are strain and dose dependent, claims should be documented in well-planned and -conducted, randomized, placebo-controlled clinical trials [37]. Moreover, translucent legislative procedures are needed for probiotics, currently classed in the nomenclature either as food or drugs.
Figure 1
Probiotics usage in case of global symptoms and abdominal pain persistence: A – meta-analysis, B – publication bias
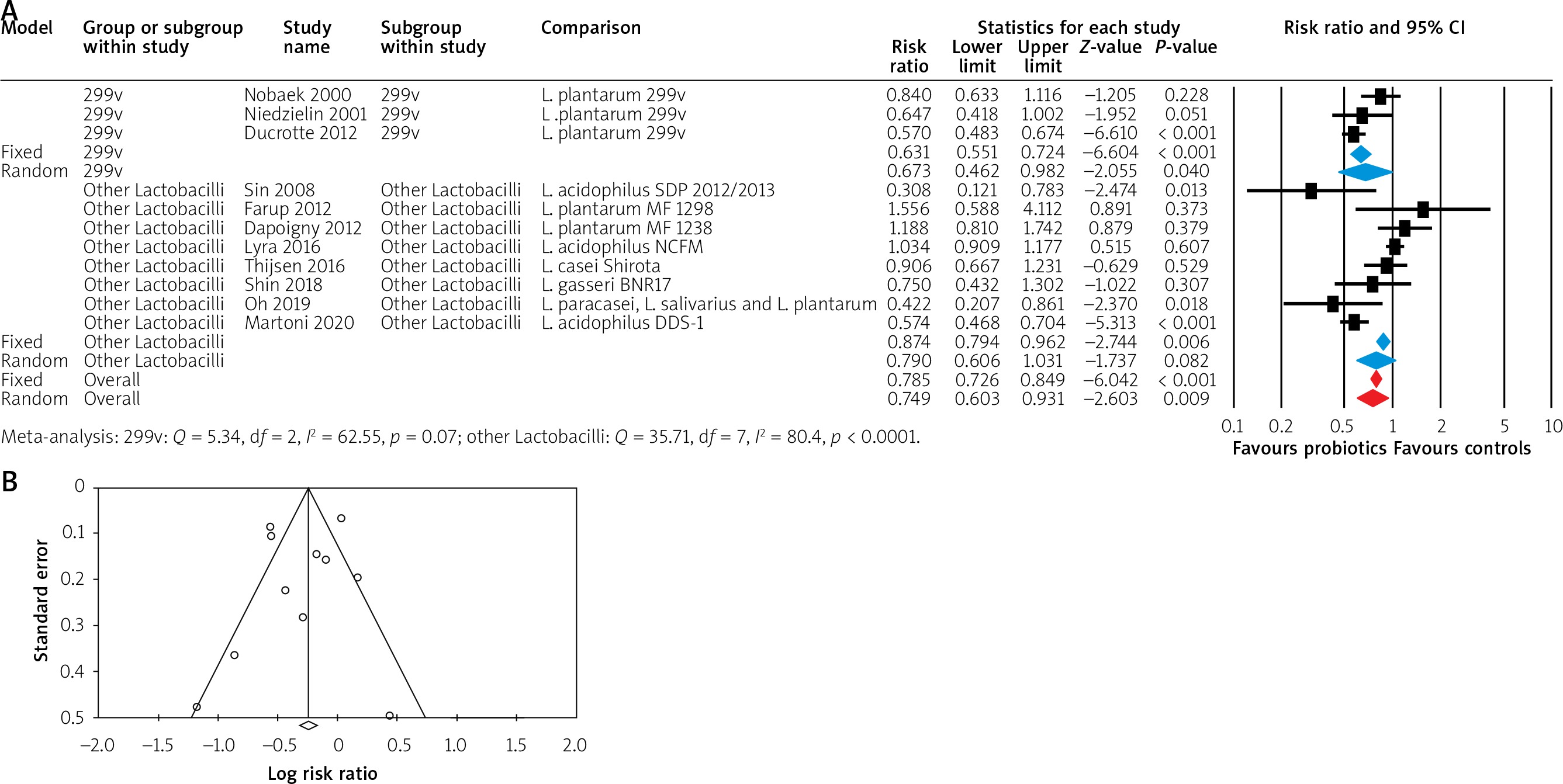
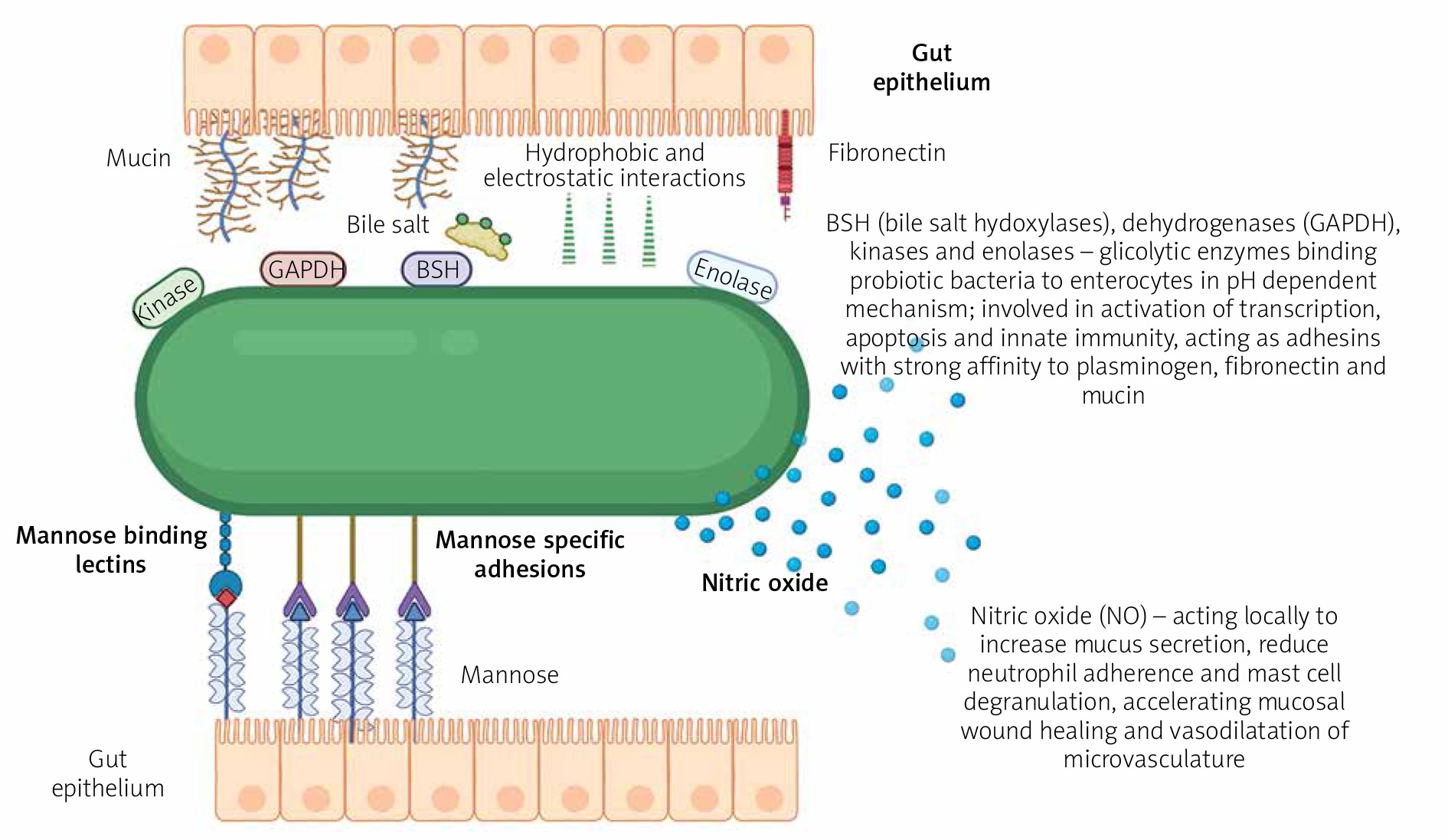
Figure 2
Adhesive properties and mechanism of action of LP299v probiotic strain [28, 30, 31]. Some mechanisms of probiotic action might be widespread; others frequently observed, yet others may be rare and characteristic for only a few strains of a given species. Evidence is mounting. Major probiotic mechanisms of action include enhancement of various elements of the epithelial barrier, increased adhesion to intestinal mucosa, concomitant inhibition of pathogen adhesion, competitive exclusion of pathogenic microorganisms, production of anti-microorganism substances, and modulation of the immune and neural systems. The main mechanisms of action of S. boulardii include inhibition of activities of bacterial pathogenic products, trophic effects on the intestinal mucosa, as well as modification of host signalling pathways involved in inflammatory and non-inflammatory intestinal diseases. The mechanism involved in anti-mutagenic activities is the ability of bifidobacteria to bind to the mutagens of microbial cells
Conclusions
Probiotics, as a group, may be an effective treatment for global symptoms and abdominal pain in patients with IBS. Subgroup analyses of available randomized clinical trials (RCTs), according to the type of probiotic used, demonstrated the strongest effects on global symptoms or abdominal pain in patients with IBS for the genus Lactobacillus, but this effect is driven by strain Lp299v. Lp299v significantly alleviates the global IBS symptoms, achieving maximum effect within 12 weeks of treatment, which is in line with the most recent and major gastrointestinal society guidelines as for the time of probiotics administration. Our current analysis is in line with previous reports documenting significant effects of Lp299v in reducing the risk of global symptoms and their persistence, which could assist clinicians in making the correct choice of probiotic strain in IBS patients [38]. Head-to-head studies evaluating the efficacy of the same or different probiotic strains in IBS patients are lacking, which stand behind limitations of various meta-analyses. Probiotics have good safety profile but require restrictive manufacturing procedures and high quality control standards.










