
Introduction
Malignant hilar biliary obstruction (MHBO) always arises as a consequence of malignant growths in the hilar hepatobiliary area [1–4]. At the time of diagnosis, MHBO patients are generally unable to undergo definite resection as the disease is often detected at an advanced stage when only palliative treatment is viable [1–4].
Metal stenting can be used as a primary treatment option for alleviating MHBO symptoms [1–6]. At present, although many studies have focused on the topic of unilateral or bilateral stenting for MHBO, it remains unclear as to which technique is preferable for treating MHBO [5–17]. Although some meta-analyses indicated that bilateral metal stenting yielded a lower rate of stent dysfunction than did unilateral metal stenting in MHBO patients [5, 9], there were many forms of bias, such as type of stents, stenting approaches, and disease types. To overcome these potential causes of bias, there is a clear need for a study comparing these two stenting types in patients with a single type of cancer.
Aim
We conducted a meta-analysis to compare the clinical efficacy of unilateral and bilateral metal stent insertion for patients affected by hilar cholangiocarcinoma (HCCA).
Material and methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement guided the conceptualization and execution of this meta-analysis. This meta-analysis was registered at https://inplasy.com/ (Number: INPLASY202110051).
Relevant studies published in the PubMed, Embase, and the Cochrane Library databases until June 2020 were identified. The search strategy adopted used the following search query: ((((unilateral[Title/Abstract]) AND bilateral[Title/Abstract])) AND stent[Title/Abstract]) AND ((biliary obstruction[Title/Abstract]) OR cholangiocarcinoma[Title/Abstract]).
Included studies met the following criteria: (a) studies comparing outcomes for unilateral vs. bilateral stenting for the treatment of HCCA; and (b) English studies.
Studies were excluded if they met any of the following criteria: (a) non-comparative studies; (b) case reports; (c) animal studies; and (d) reviews.
Data extraction
Two investigators independently extracted data (authors, publication year, baseline patient characteristics, study design, and treatment information) from all studies. Any discrepancies found in the extracted data were resolved by the corresponding author.
Quality assessment
The 8-point Jadad composite scale was utilized to evaluate randomized controlled trial (RCT) quality [17]. All non-RCTs were evaluated with the 9-point Newcastle-Ottawa scale [18].
Endpoints and definitions
Analyzed endpoints included rates of technical success, clinical success, complications, stent dysfunction, and overall survival.
Technical success was defined by successful stent placement beyond the obstructed site such that contrast media could pass easily through the stent. Clinical success was defined by a ≥ 30% decrease in total bilirubin levels within 2 weeks after stenting or a 50% reduction within 4 weeks [13–16]. Stent dysfunction was anything that resulted in reobstruction or stent migration [13–16]. Overall survival (OS) was defined as the time from stent implantation to death.
Statistical analysis
RevMan v5.3 was used for all data analyses. The Mantel-Haenszel approach was used for calculating pooled odds ratios (ORs) and 95% confidence intervals (CIs) for dichotomous variables. Overall survival was assessed using hazard ratios (HRs) with 95% CIs. Heterogeneity was measured using the X2 and I2 tests, with I2 > 50% indicating significant heterogeneity. When significant heterogeneity was not present, analysis was performed using a fixed-effects model. Potential heterogeneity sources were evaluated using sensitivity and subgroup analyses, while funnel plots were used to assess potential publication bias.
Results
Study characteristics
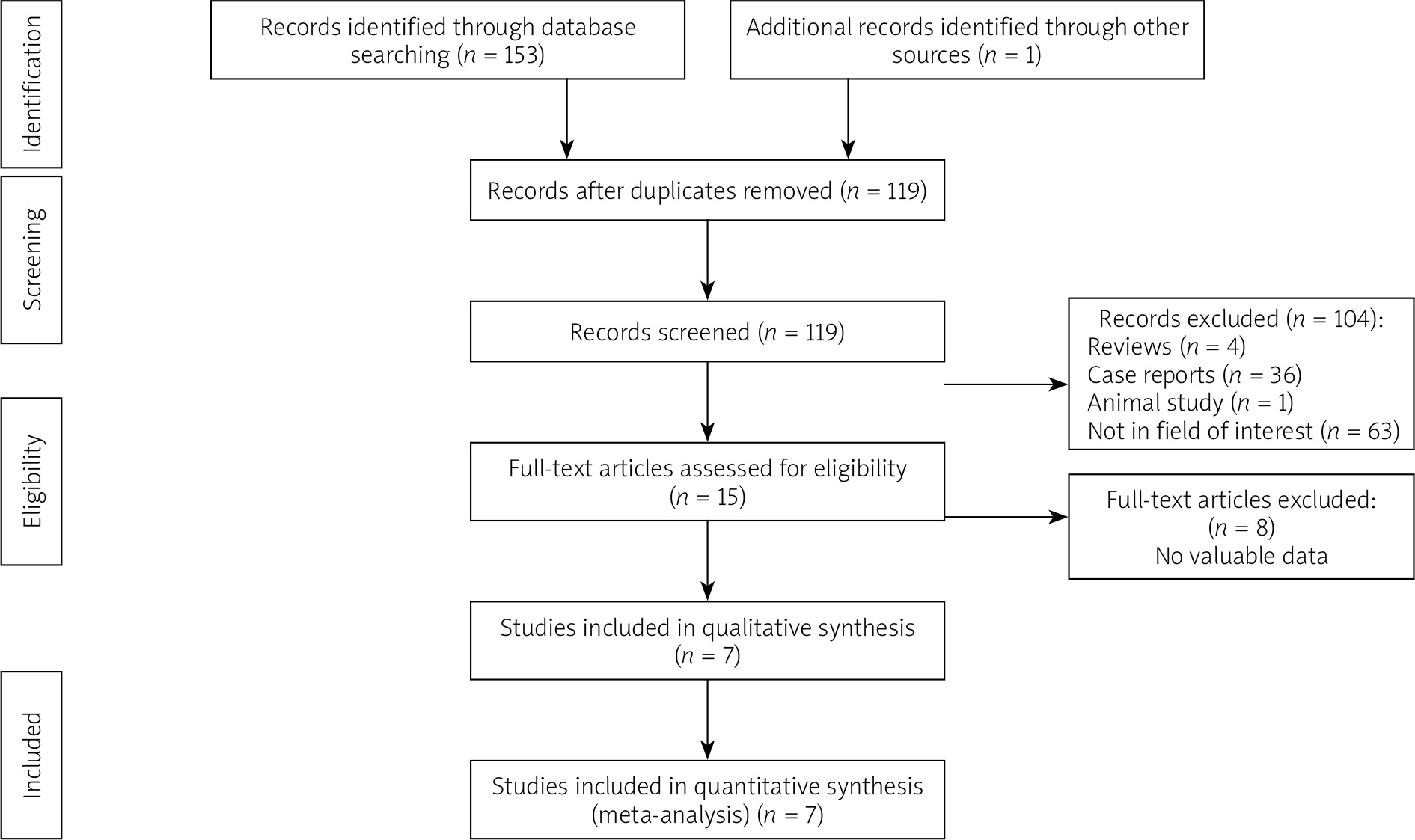
We initially identified 154 studies, seven of which were included in this meta-analysis (Figure 1). Six were retrospective studies [11–15, 17], while one was an RCT [16]. In total, these studies included 524 HCCA patients treated by either unilateral (n = 215) or bilateral (n = 309) stenting.
Details of included studies are shown in Tables I and II. The related data were directly extracted from 5 studies [11, 12, 14, 15, 17]. Two studies did not directly report the data of HCCA patients, and we obtained the data by contacting the corresponding authors of these articles [13, 16]. Endoscopic stenting was performed in three studies [11, 12, 17], whereas percutaneous stenting was conducted in four studies [13–16]. The 6 retrospective studies were evaluated as Newcastle-Ottawa scale 5-8. The 1 RCT was evaluated as Jadad scale 5.
Table I
Characteristics of the included studies
| Study/year/country | Study design | Bismuth | Groups | Sample size | Age [years] | Jadad scale | NOS |
|---|---|---|---|---|---|---|---|
| Naitoh/2009/Japan [11] | Retrospective | I-IV | Unilateral | 6 | – | – | 5 |
| Bilateral | 9 | – | |||||
| Liberato/2012/Portugal [12] | Retrospective | II | Unilateral | 35 | – | – | 6 |
| Bilateral | 42 | – | |||||
| Chang/2017/China [13] | Retrospective | II-IV | Unilateral | 23 | 63.3 | – | 8 |
| Bilateral | 23 | 68.5 | |||||
| Yin/2019/China [14] | Retrospective | II-IV | Unilateral | 51 | 64.3 | – | 8 |
| Bilateral | 42 | 68.5 | |||||
| Teng/2019/China [15] | Retrospective | II-IV | Unilateral | 33 | – | – | 5 |
| Bilateral | 35 | – | |||||
| Fu/2019/China [16] | RCT | II-IV | Unilateral | 17 | 65.2 | 5 | – |
| Bilateral | 21 | 64.3 | |||||
| Staub/2020/Multicenter [17] | Retrospective | I-IV | Unilateral | 50 | 73.1 | – | 7 |
| Bilateral | 137 | 72.1 |
Table II
Characteristics of treatments
| Study | Deployments | Approaches | Groups | TS | CS | SD | Complications |
|---|---|---|---|---|---|---|---|
| Naitoh [11] | Side-by-side | Endoscopic | Unilateral | Not given | Not given | 3/6 (50%) | Not given |
| Bilateral | Not given | Not given | 2/9 (22.2%) | Not given | |||
| Liberato [12] | Side-by-side, stent-in-stent | Endoscopic | Unilateral | 35/35 (100%) | Not given | 11/35 (31.4%) | Not given |
| Bilateral | 42/45 (93.3%) | Not given | 5/42 (11.9%) | Not given | |||
| Chang [13] | Side-by-side | Percutaneous | Unilateral | 22/23 (95.7%) | 21/22 (95.4%) | 2/22 (9.1%) | 1/22 (4.5%) |
| Bilateral | 23/23 (100%) | 23/23 (100%) | 1/23 (4.3%) | 3/23 (13.0%) | |||
| Yin [14] | Side-by-side | Percutaneous | Unilateral | 47/51 (92.2%) | 45/47 (95.7%) | 6/47 (12.8%) | 3/47 (6.4%) |
| Bilateral | 40/42 (95.2%) | 38/39 (97.4%) | 3/40 (7.5%) | 5/40 (12.5%) | |||
| Teng [15] | Side-by-side | Percutaneous | Unilateral | Not given | 32/33 (97.0%) | Not given | Not given |
| Bilateral | Not given | 34/35 (97.1%) | Not given | Not given | |||
| Fu [16] | Side-by-side | Percutaneous | Unilateral | 15/17 (88.2%) | 14/15 (93.3%) | 2/15 (13.3%) | 2/15 (13.3%) |
| Bilateral | 18/21 (85.7%) | 18/18 (100%) | 1/18 (5.6%) | 1/18 (5.6%) | |||
| Staub [17] | Not given | Endoscopic | Unilateral | 50/50 (100%) | Not given | 21/50 (42%) | 0/50 (0%) |
| Bilateral | 137/137 (100%) | Not given | 60/137 (43.8%) | 16/137 (11.7%) |
Technical success
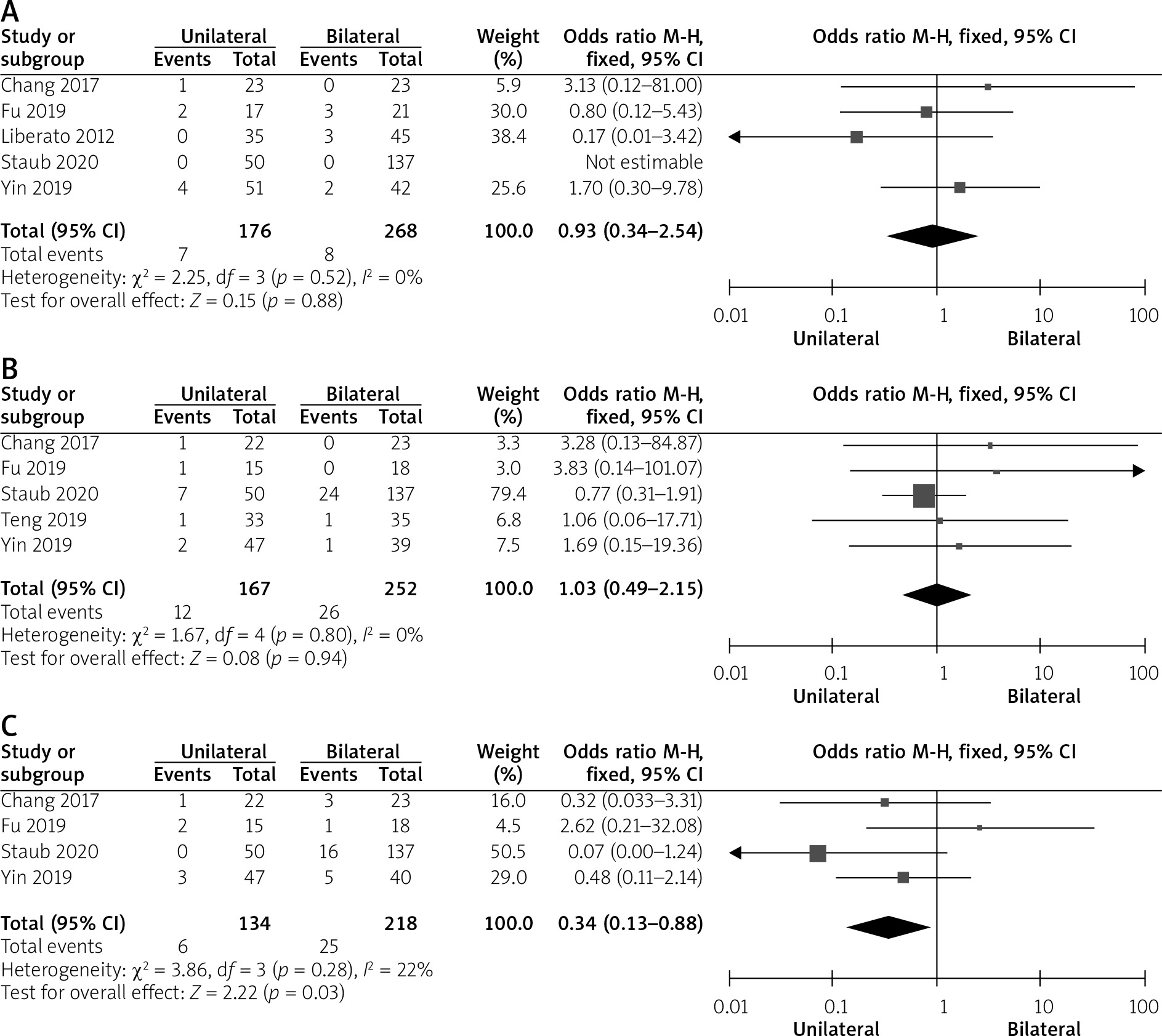
Technical success rates could be obtained from five studies [12–14, 16, 17]. No significant heterogeneity was detected (I2 = 0%; p = 0.52, Figure 2 A). The pooled technical success rates of unilateral and bilateral stenting were 96% and 97%, respectively (OR = 0.93; 95% CI: 0.34–2.54, p = 0.88).
Clinical success
Data regarding rates of clinical success could be obtained from five studies [13–17]. No significant heterogeneity was seen (I2 = 0%; p = 0.80, Figure 2 B). The pooled rates of clinical success of unilateral and bilateral stenting were 92.8% and 89.7%, respectively (OR = 1.03; 95% CI: 0.49–2.15, p = 0.94).
Complications
Complication data could be obtained from four studies [13, 15–17]. No significant heterogeneity was seen (I2 = 22%; p = 0.28, Figure 2 C). The pooled rates of complication of unilateral and bilateral stenting were 4.5% and 11.5%, respectively (OR = 0.34; 95% CI: 0.13–0.88, p = 0.03).
Stent dysfunction
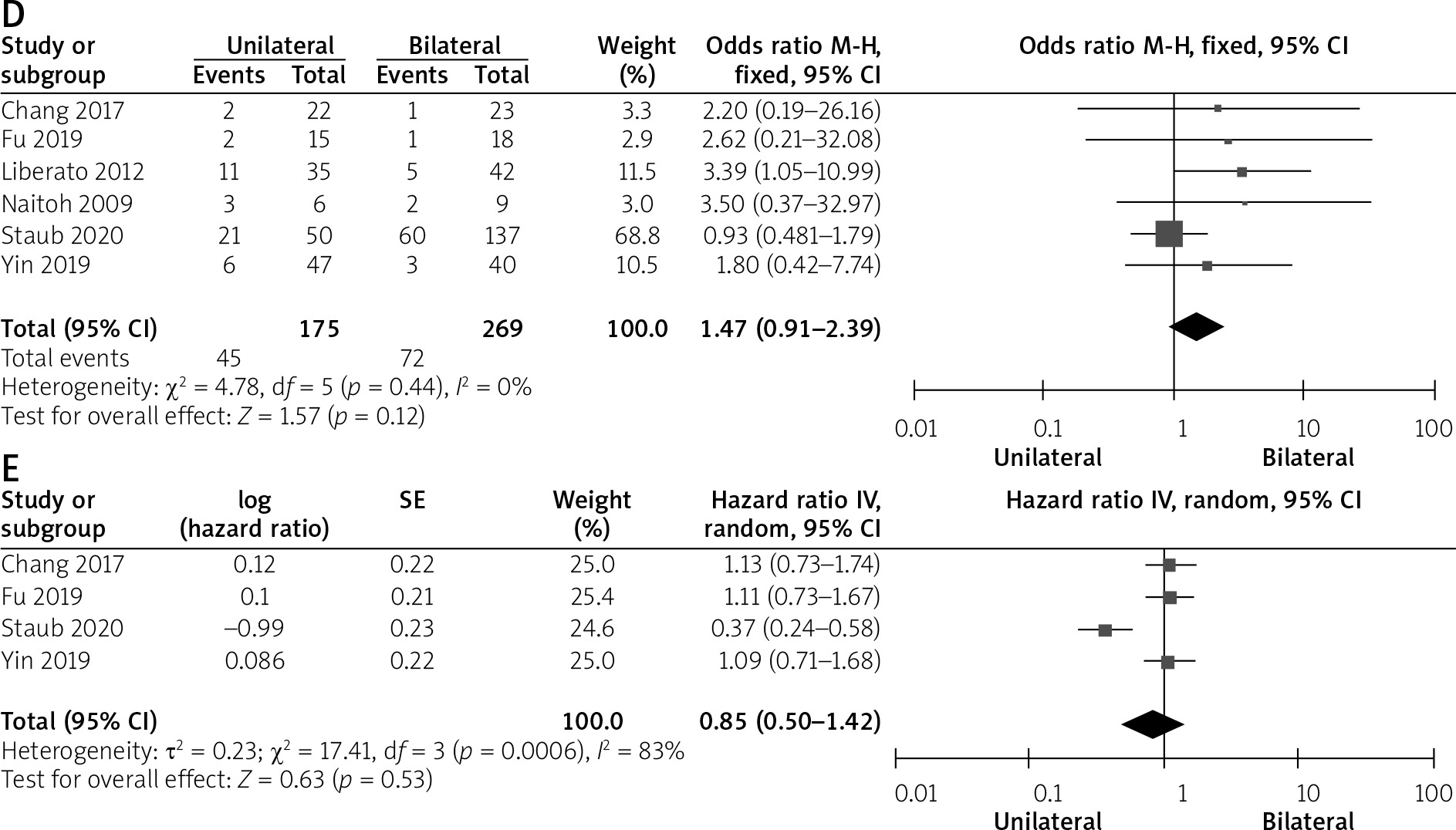
Stent dysfunction rates were available from six studies [11–14, 16, 17]. No significant heterogeneity was detected (I2 = 0%; p = 0.44, Figure 2 D). The pooled rates of stent dysfunction of unilateral and bilateral stenting were 25.7% and 26.7%, respectively (OR = 1.47; 95% CI: 0.91–2.39, p = 0.12).
Overall survival
Overall survival could be extracted from four studies [13, 14, 16, 17]. Significant heterogeneity was detected (I2 = 83%; p = 0.0006, Figure 2 E). Overall survival did not differ significantly between the 2 groups (HR = 0.85; 95% CI: 0.50–1.42, p = 0.53). The sensitivity analysis revealed that the source of heterogeneity was the Staub study [17].
Subgroup analysis
Table III shows the pooled stent dysfunction rates based on the use of endoscopic or percutaneous stenting. Significant heterogeneity was detected in the subgroup of endoscopic stenting (I2 = 54%). The difference between the 2 groups based on the 2 subgroups was not significant.
Discussion
HCCA is the most common cause of MHBO [11–17]. Metal stents currently represent a standard treatment for MHBO, as they offer greater advantages in terms of clinical success, stent patency, and patient survival than do plastic stents [10]. However, it has remained controversial as to whether MHBO or HCCA is best managed via unilateral or bilateral stenting.
Unlike previous meta-analyses regarding unilateral vs. bilateral stenting for MHBO [5, 9, 19, 20], this meta-analysis solely focused on HCCA. We observe no significant differences in either technical (p = 0.52) or clinical (p = 0.80) success when comparing patients treated via unilateral and bilateral metal stenting, consistent with previous meta-analyses regarding treating MHBO via percutaneous or endoscopic stenting [5, 9]. Unilateral stent insertion is sufficient to relieve MHBO-associated jaundice, as TBIL levels can be normalized by facilitating the drainage of just 25–30% of the liver [12].
A meta-analysis regarding of endoscopic unilateral vs. bilateral metal stenting for MHBO indicated a significant higher technical success rate in the unilateral group [20]. In our meta-analysis, four studies used percutaneous stenting [13–16]. Compared to the endoscopic approach, percutaneous stenting for MHBO is easier, as the distance from puncture site to obstructed site is very short.
In this meta-analysis, we found a significantly higher complication rate in the bilateral group (11.5% vs. 4.5%, p = 0.03). Six included studies reported the use of side-by-side technique of bilateral stenting, which necessitates the insertion of two stents into the common biliary tract. This can induce higher levels of compressive stress on the biliary wall, thereby potentially increasing the risk of cholangitis.
A significant lower bilateral stent dysfunction rate was found in the previous studies regarding unilateral vs. bilateral stenting for MHBO [5, 9]. However, our meta-analysis demonstrated similar stent dysfunction rates between 2 groups (25.7% vs. 26.7%, p = 0.12). This finding may be related to the following factors: (a) the HCCA is a subtype of MHBO, therefore, the sample size decreases; and (b) six of the 7 included studies were retrospective in design and may thus be affected by selection bias. The subgroup analysis still revealed similar stent dysfunction rates between the 2 groups based on the percutaneous or endoscopic approaches. Further high quality studies are still required to confirm this finding.
We observed similar OS between the 2 groups (p = 0.53), which may be because some of the patients included in the present meta-analysis were from studies in which stenting was employed as a post-operative anti-cancer treatment [13, 14, 16]. While such stenting can relieve jaundice in HCCA patients, it cannot directly impact the primary malignancy. Instead, further anti-cancer treatments are necessary to extend patient survival in these cases [21].
There are a number of limitations to the present meta-analysis. First, the majority of the studies included herein were retrospective in nature, thus introducing the potential for selection bias. Second, the studies included in the present meta-analysis used a number of different stent insertion approaches, including percutaneous and endoscopic approaches, thus potentially further biasing these results. Third, many endpoint data were lost in many included studies, thus potentially constraining the applicability of our findings.










