
A 65-year-old woman was referred to the Department of Internal Medicine due to severe microcytic anaemia. She complained of progressive fatigue for the past 4 months. Clinical examination revealed pallor and tenderness to palpation in the upper abdomen; per rectum examination did not reveal any signs of active gastrointestinal bleeding. Laboratory tests demonstrated substantial iron-deficiency anaemia with haemoglobin and iron levels of 6.8 g/dl (norm: 12.3–16 g/dl) and 12 µg/dl (norm: 33–193 µg/dl), respectively, and MCV 66.5 fl (norm: 81–101 fl). Other serum parameters, including the concentration of gastrointestinal tumour markers and coagulation panel, remained within the reference range. Her medical history was relevant for upper-gastrointestinal bleeding, oesophagitis grade B in LA classification , Helicobacter pylori infection, and hypertension. She had previously been repeatedly hospitalized for symptomatic microcytic anaemia with the need for blood transfusions and IV iron infusions because she did not tolerate oral iron supplementation.
The patient was admitted and transfused with 3 units of packed red blood cells. Esophagogastroduodenoscopy was performed; however, it could not be completed due to the lack of the possibility to pass beyond the body of the stomach (Figure 1 A). Contrast examination of the upper gastrointestinal tract was proposed, to assess the location of the stomach. It identified a large hiatal hernia with the whole stomach located above the diaphragm, as well as the twist of the stomach with the body and antrum localized above the fungus (Figure 1 B). The patient underwent Nissen fundoplication – in a control contrast study, anatomical localization of the stomach was confirmed (Figure 1 C). Three months later her iron deficiency completely resolved, her haemoglobin level returned to normal, and her well-being improved. Control laboratory indices were as follows: HGB 13.6 g/dl, MCV 84.3 fl, iron: 182 µg/dl, transferrin: 2.85 g/l (norm: 2–3.6 g/l), ferritin: 24.10 ng/ml (norm: 4.633–200 ng/ml), B12: 222 pg/ml (norm: 197–771 pg/ml), and folic acid: 6.63 ng/ml (norm: 3.10–17.50 ng/ml). She has not required iron supplementation since the surgery.
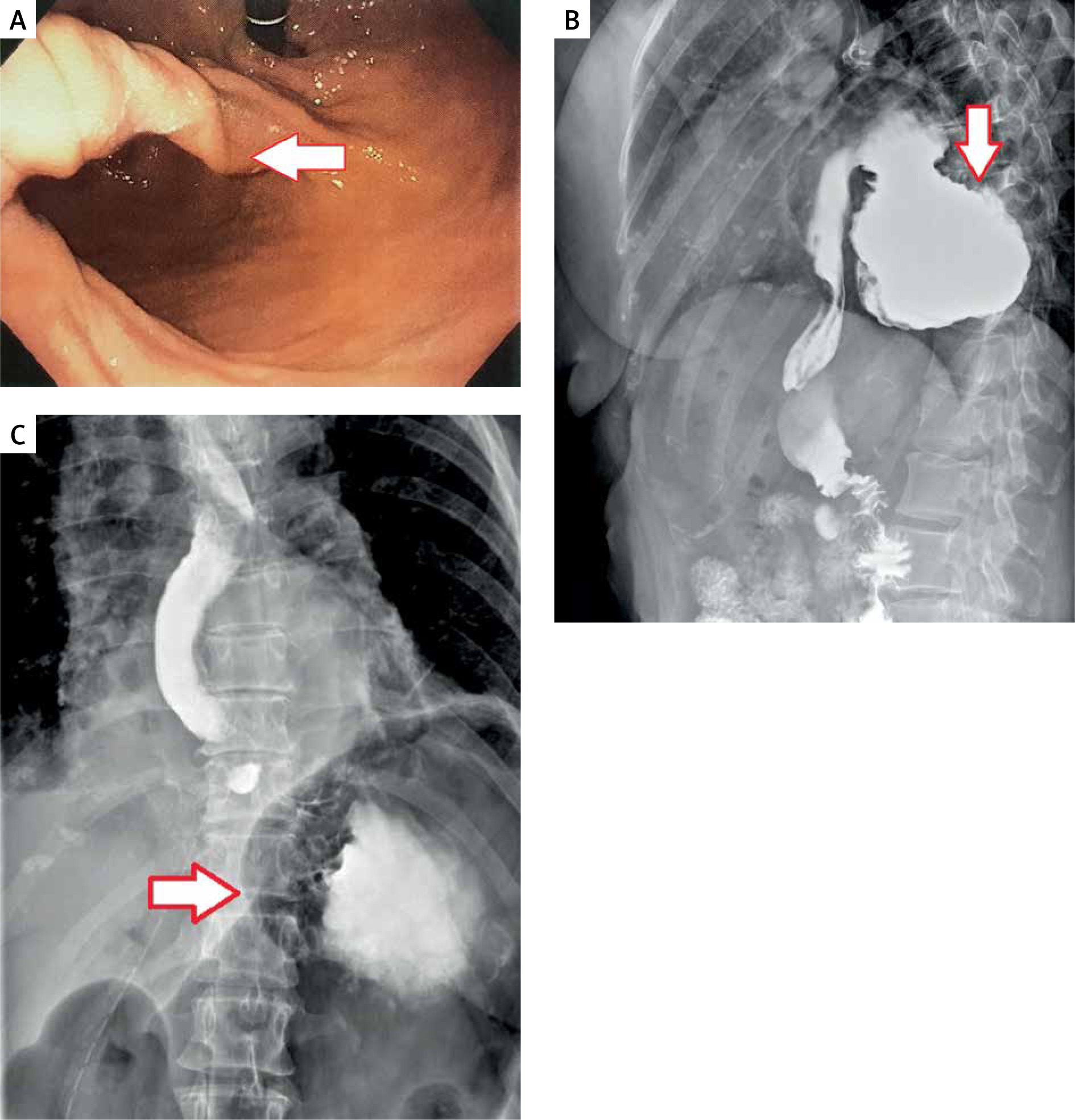
Figure 1
A – gastroscopy showing twist of the stomach with an endoscope unable the pass further. B – contrast X-ray of the GI tract showing a giant hiatal hernia. C – contrast X-ray of the GI tract after hernia repair with Nissen fundoplication, showing anatomical location of the stomach
We believe that the most likely underlying cause of the above case is the presence of Cameron lesions or, in its more severe form, Cameron ulcers. These are erosions mostly found on the lesser curvature of the stomach, at the neck of the hiatal hernia. They form due to chronic ischaemia at the site of the hernia sliding through the diaphragm [1] and can result in chronic, occult gastrointestinal bleeding. Some studies show that a mean of 45% patients with giant hiatal hernia have iron-deficiency anaemia [2, 3]. It is worth noting is that as many as 90% of the patients with symptomatic anaemia and hiatal hernia can have their symptoms resolved after surgical treatment, and there is usually no need for further oral supplementation of iron following the procedure [3, 4]. Clinicians should always consider operative management in patients with persistent, symptomatic iron-deficiency anaemia and co-existing hiatal hernia, because such intervention greatly improves their quality of life.










