
Introduction
Inflammatory bowel diseases (IBD) are chronic disorders of the gastrointestinal tract with a remitting-relapsing disease pattern. Ulcerative colitis (UC) and Crohn’s disease (CD) represent the two main forms of IBD with a dissimilar disease extension: only the large intestine for UC and all of the digestive tract for CD. In CD inflammation affects various parts of the bowel, separated by unchanged intestinal segments, while in ulcerative colitis enteric involvement is continuous, extending from the rectum throughout the colon. Additionally, in Crohn’s disease the inflammatory process spreads through all layers of the intestinal wall, while in UC only the mucosa and submucosa are affected. Both disease entities have a complex and still partially unknown aetiology involving environmental factors, and autoimmune together with genetic characteristics. The diagnosis of IBD is based on clinical presentation, laboratory tests, imaging techniques, and endoscopic examination with histopathology findings. The increasing incidence of UC and CD, the prevalence in the group of children and young adults, as well as a lifelong disabling character of these conditions, require a search for the most adequate and convenient imaging technique.
The aim of this article is to present, based on current literature, the utility of different radiological techniques for IBD, with a consideration of their effectiveness and radiation exposure.
The radiological techniques used in inflammatory bowel diseases
Plain radiography
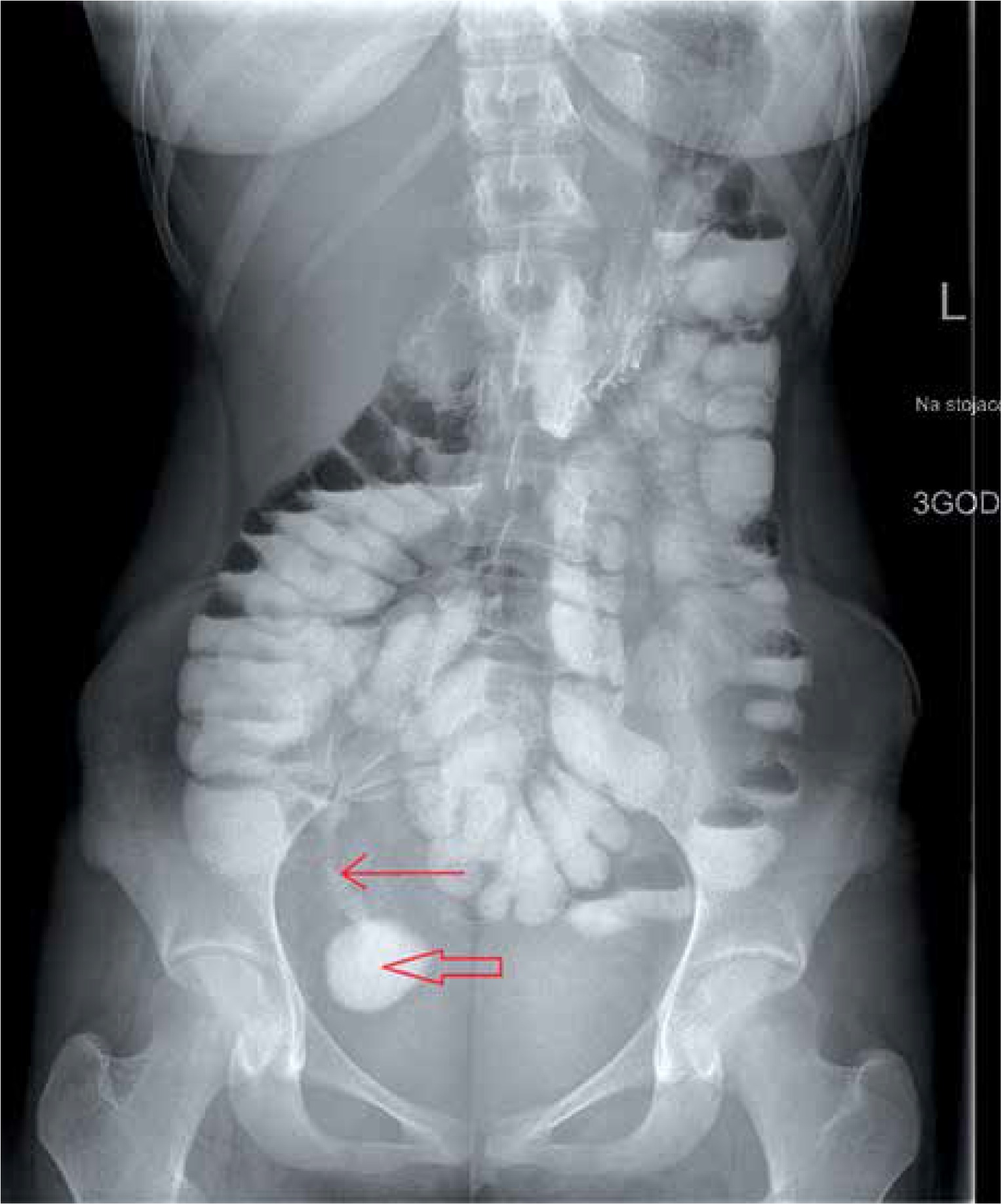
Abdominal X-ray is a low-cost examination, widely used in internal medicine, gastroenterology, and emergency units. Its availability and rapid evaluation of the image are suitable for acute situations like intestinal obstruction, shown as dilated bowel loops with air-fluid levels (Figure 1) or perforation, represented as a free intra-abdominal gas. According to ECCO guidelines, plain film radiography enables detection of small bowel obstruction in stricturing CD. However, the findings from radiography should be followed by further diagnostic study using ultrasonography or other cross-sectional imaging techniques [1]. To exclude a perforation both upright and supine projections should be performed. For patients who cannot maintain a standing position, left lateral decubitus positioning is recommended [2]. Other abnormalities that can be detected by a plain radiography are: toxic megacolon and colonic haustrations loss. Toxic megacolon constitutes a severe complication, more frequent in UC than in CD. It can be diagnosed by an abdominal X-ray as a colonic dilatation larger than 6 cm in the presence of clinical signs of toxicity [3]. In conclusion, the role of plain radiograms in the assessment of IBD can be defined as a first-line examination of acute, life-threatening complications.

Barium contrast studies
Barium studies consist of X-ray series performed during a contrast passage through the gastrointestinal tract. In IBD, two major techniques are used: barium enema (BE) with barium contrast administrated rectally and small bowel follow- through with an oral contrast. Barium enema is performed to demonstrate colonic involvement of IBD. The examination is based on the use of single (barium sulphate) or double contrast (high-density barium as a positive contrast and air or carbon dioxide as a negative contrast). In the double-contrast barium enema, the air insufflation provokes bowel distension. A barium sulphate layer covers the intestinal mucosa showing its irregularities, erosions, and ulcers, which create an image of “stippling of paint” [2]. Small bowel follow-through (SBFT) used to be a key radiological technique to detect CD located in the small bowel [4]. After overnight fasting, a contrast is administrated orally, swallowed by the patient or via a nasogastric tube preferably positioned beyond the duodenojejunal angle – small bowel enteroclysis (SBE). The CD features that can be detected by SBFT are: wall thickening and stenotic lesions [5] (Figure 2). Contrast studies with barium are contraindicated if perforation is suspected. In these cases, a water-soluble contrast can be used.
Figure 2
A small bowel follow-through of a 25-year-old woman with CD, showing a contrast deposition in the right iliac fossa (closed arrow), representing a dilated bowel loop with a distal stricture (open arrow); picture taken 3 h after contrast administration
Nowadays, the role of BE and SBFT is reduced due to the considerable radiation exposure in addition to a lower sensitivity in comparison with CT and MR enterography for extra-luminal complications and small bowel disease [6, 7]. The ECCO guidelines for CD recommend therefore the use of cross-sectional techniques instead of conventional barium series [1].
Ultrasonography
Another easily accessible and low-cost technique, useful in IBD management, is ultrasonography (US). It allows a real-time diagnosis with no radiation exposure. No special bowel preparation is needed except for 6 h fasting before the procedure to minimise the intestinal air content [2]. The US images that can be found in CD and UC are: bowel wall thickening (greater than 3 mm for colon and greater than 2 mm for small intestine), pseudostratification, inflammatory mass, and loss of colonic haustration [8]. This technique enables the assessment of IBD complications, such as strictures, abscesses, and fistulas as well as other extraluminal manifestations, such as lymph node enlargement and changes in the appearance of the mesenteric adipose tissue (creeping fat). In an Israeli study the sensitivity of bowel ultrasound for mural thickening and IBD complications was compared to the results from the imaging techniques considered as a gold standard: computed tomographic enterography, magnetic resonance enterography, and colonoscopy. The IBD features were detected by US with the following sensitivity: 90% for the bowel wall thickening, 94% for stenosis, and 75% for inflammatory mass [8].
There is a need to search for modalities improving the potential of US to identify IBD-related lesions. Doppler ultrasound demonstrates an increased vascularity due to the inflammatory process in the bowel wall. Oral (small-intestine contrast-enhanced ultrasonography – SICUS) and intravenous contrast (contrast-enhanced ultrasonography – CEUS) are used for better visualisation of the bowel wall and for increased diagnostic accuracy of US. In conventional ultrasonography the main limitations are intestinal gas and bowel wall collapse, which both reduce the visualisation of bowel pathologies. Oral contrast administration before the procedure helps to eliminate the negative effects of endoluminal air and enables bowel distension. Small-intestine contrast-enhanced ultrasonography is superior (sensitivity: 96.1%) to US (sensitivity: 91.4%) in small bowel CD diagnosis [9]. Intravenous contrast, administrated during ultrasonography, enhances the ability to differentiate between active disease and fibro-stenotic complications. Contrast-enhanced ultrasonography was proven to be useful in IBD follow-up and disease recurrence detection [10].
To summarize, abdominal US is a non-invasive, inexpensive, and well-tolerated examination technique. The use of colour Doppler and contrast increases the accuracy of US to present disease location and activity.
Computed tomography
Because of its availability and rapid image acquisition, abdominal computed tomography (CT) is one of the first-line imaging modalities in IBD patients. It is especially effective in recognition of extraluminal complications, like fistula (Figure 3) or abscess and extraintestinal manifestations such as: cholelithiasis, pancreatitis, nephrolithiasis, sacroiliitis, and primary sclerosing cholangitis. Computed tomography is also performed when intestinal obstruction or perforation are suspected. Bowel wall pathologies detected by CT with intravenous contrast are: thickening, mucosal enhancement, and stratification. Despite its utility mentioned above, conventional CT scanning in IBD has some limitations. Firstly, there is a high radiation exposure, which constitutes a major issue because IBD relapses involve repetitive radiological examinations. Secondly, small intestine imaging in the standard CT is altered by the collapsed loop artefacts [4]. To increase the visibility of small bowel lesions, the technique of CT enterography (CTE) was introduced. The method is based on CT scanning with intravenous and enteral contrast. While routine CT is used especially to detect the extraluminal complications of IBD, CT enterography effectively presents bowel inflammation. An intravenous contrast provides a better illustration of inflammatory bowel disease features: hyperenhancement and thickening of intestinal wall [11], whereas low-density or neutral oral contrast agents (polyethylene glycol, water–methylcellulose solution, or mannitol solution) stimulate luminal distension [11, 12]. There are two ways to administer a contrast solution: either drunk by the patient before the procedure (CT enterography) or provided through a nasojejunal tube placed distally to the ligament of Treitz. In the latter case, the term of computed tomographic enteroclysis is used. In addition to the use of contrast, patient preparation consists of fasting at least 4 h before the exam and intravenous or intramuscular administration of an antispasmodic drug (hyoscine butylbromide) prior to CTE scanning in order to minimise bowel peristalsis [12]. Additionally, if colonic lesions are suspected, a bowel cleansing and insufflation with air via rectal tube may be performed – CT colonography [12]. The main radiological features of IBD, concerning the bowel wall as well as perienteric fat and lymph nodes, which can be detected in CTE are summarised in Table I. The management of IBD requires multiple radiological procedures for diagnosis establishment and confirmation, assessment of the disease severity and activity, evaluation of the response to therapy, and finally estimation of the need for surgical treatment. The utility of CTE has been demonstrated in all the situations enumerated above [12, 13]. A distinction between an active CD or UC and fibrostenotic lesions constitutes a challenge for radiological techniques. In CT enterography the active CD demonstrates principally as mural hyperenhancement and bowel wall thickening [14]. As for the chronic disease, it is represented in CTE by strictures and absence of increased enhancement, fibrofatty proliferation, hyperaemia, or oedema.
Figure 3
The CT axial scan of a 19-year-old woman with CD, showing an inflammatory infiltrate in pelvis (open arrow) with an atypical air collection adjacent to infiltrated sigmoid and jejunum loops (filled arrow) – suspicion of a fistula
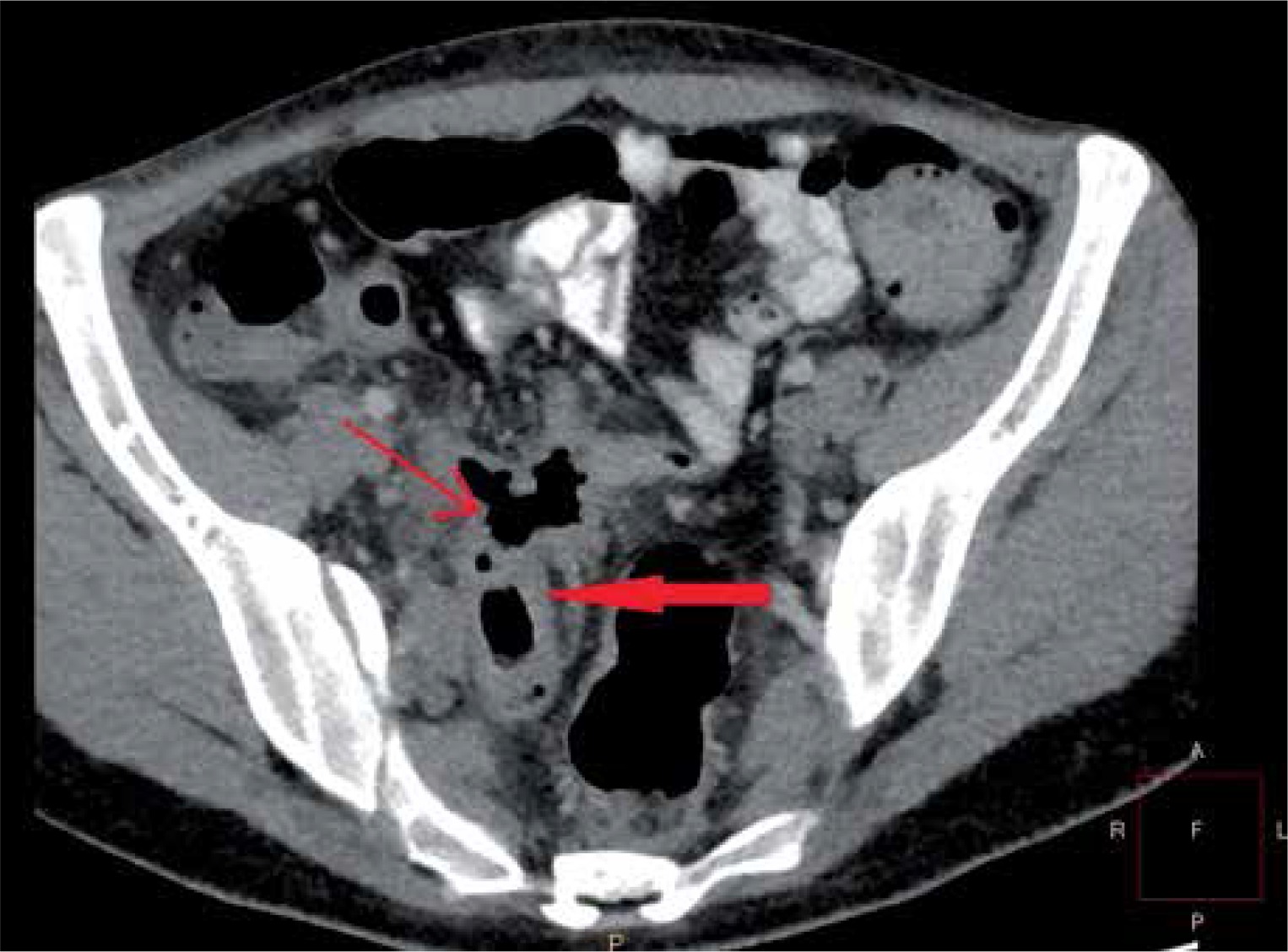
Table I
Radiologic features of inflammatory bowel disease in CTE
To conclude, routine CT is used to detect severe complications and extraintestinal manifestations, whereas CTE depicts IBD activity and bowel wall involvement. Given the significant radiation exposure, the use of computed tomography scanning has to be restricted to urgent conditions.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is a non-ionising, cross-sectional technique, increasingly used in recent years. Its utility in the assessment of gastrointestinal tract diseases is limited by high cost, reduced availability, and considerable duration of the procedure, when compared to other radiological examinations [15]. However, because of its potential for small bowel imaging, magnetic resonance enterography (MRE) constitutes an approved radiological method for IBD patients. Additionally, MRI of the perineum is an effective tool for perineal disease presentations: local lymphadenopathy, intersphincteric, trans-sphincteric, and internal fistulas, perineal abscess, and sinus tracts [16]. As specified in the ECCO guidelines 2016 for CD, MRE, if available, should be the exam of choice for the diagnostic process and management of the disease. This recommendation is due to the lack of radiation in magnetic resonance imaging and its similar capacity to show extension and activity of CD when compared to CT [1]. The preparation for MRE, as in the case of CTE, requires a 4 to 6 h of fasting before the examination and use of an oral contrast, drunk by the patient or distributed by a nasojejunal tube (magnetic resonance enteroclysis). There are a wide range of contrast agents that are used to stimulate bowel distension: polyethylene glycol solution (PEG), sorbitol, mannitol, or lactulose water solution. Additionally, an intravenous spasmolytic (e.g. butylscopolamine bromide, hyoscine butylbromide, or glucagon) diminishes peristalsis for a better bowel visualisation. Another similarity with CTE protocol is the use of intravenous (IV) contrast in order to improve the sensitivity for intestinal wall abnormalities [17]. The findings in MR enterography are analogous to the features detected by CTE: bowel wall thickening and hyperenhancement, lymphadenopathy, hypervascularity, fibrofatty proliferation, abscesses, fistulae, and stenosis (Figures 4 and 5) [18]. Multiple studies analysed the potential of MRE for IBD. As specified in an Israeli study [19], MRE was as successful as small-bowel video capsule endoscopy (VCE) in reforming the initial Montreal classification of CD patients: 47% of changed disease classifications for MR enterography and 45.5% for endoscopic findings. Another study compared the two modalities (MRE and VCE), given the patients acceptance and preference [20]. The necessity of contrast ingestion was the main inconvenience of MRE when compared to VCE preparation. The conclusions of the study reveal patients’ tolerance as a significant difficulty in IBD management and follow-up.
Figure 4
MRE scan in T2W TSE coronal BH sequence of the patient from Figure 1 showing an inflammatory infiltrate alongside right ileum wall constricting the right ureter and provoking retention in the right pelvicalyceal system

Figure 5
MRE axial scan in mDIXON sequence of a young woman with CD showing a thickened wall of sigmoid and descendent colon with a luminal stricture

Because it permits avoidance of radiation exposure, magnetic resonance imaging in CD and UC patients appears to be especially favourable in the paediatric population. On the other hand, the need for optimal patient compliance during the contrast administration and breath-hold sequences, as well as the increased risk of motion artefacts, are essential challenges for MRE in children with IBD [15]. To reduce the negative influence of MRI characteristics (long procedure time, high cost, patient adherence) on the choice of examination technique, Danish researchers tended to establish the best magnetic resonance imaging protocol for IBD patients [21]. They compared the accuracy of plain MRI with no contrast administration, magnetic resonance using oral and intravenous contrast agents, and MR enteroclysis with contrast given through a nasojejunal tube. As stated in the results, the ability of MRI to detect intestinal lesions increases with the administration of both intravenous and oral contrasts. British researchers investigated the impact of diffusion-weighted images (DWI) on the accuracy of MRE in reporting the IBD activity [22]. In the DWI technique images are generated from the data established in free motion of water. Thus, inflammation results in restriction of diffusion. Moreover, an abnormal DWI signal correlates with the calprotectin level being a marker of bowel inflammation [22]. Another study analysed the effect of DWI on diagnosis of active IBD lesions when compared to gadolinium-enhanced MRE in children [23]. Diffusion-weighted images had higher sensitivity, especially for terminal ileum and ileo-caecal junction region. Furthermore, DWI does not require use of a contrast, the sequence is shorter and can be effectuated in free-breathing, leading to a better tolerance, which is especially important in young patients. Despite the qualities of DWI, the MRE protocol with contrast has a greater spatial resolution and is indispensable in the recognition of abscess and fistulas.
To sum up, magnetic resonance imaging has become one of the standard techniques in the diagnostic process and monitoring of IBD extent and activity, MR enteroclysis and enterography remaining the best magnetic resonance modalities to demonstrate transmural and extramural involvement.
Discussion
One of the tasks of imaging modalities in IBD management is to detect and confirm a remission. Mucosal healing has become the supreme treatment target in IBD. Tools like the Crohn’s disease activity index (CDAI) and biochemical markers, such as C-reactive protein or faecal calprotectin, are imperfect at revealing colonic inflammation. Repeated endoscopies are invasive and inconvenient for the patients. Therefore, there is still a need for a technique that depicts, with the best accuracy, the inflammatory activity in the mucosa. A study compared the ability of video capsule endoscopy and MRE to show small bowel inflammation in CD, evaluated by quantitative methods [24]. Magnetic resonance enterography was demonstrated as effective to present extraluminal complications of CD, as well as intraluminal inflammation and oedema. Its role was limited in cases of mild and moderate inflammation of mucosa, detected by VCE. Finally, endoscopic examination of the bowel remains an inevitable and the most valuable tool for subtle changes in the mucosal layer, magnetic resonance enterography playing a complementary role in the diagnosis and monitoring of CD. These findings harmonise with ECCO guidelines assigning to MRE, CTE, and trans-abdominal ultrasonography a supportive role, after endoscopy as a leading modality, in the detection and staging of CD [1]. In addition to this, ECCO agreed that CTE and MRE are the current standards for small intestine assessment, showing the extension and activity of CD. As for the evaluation of penetrating complications, like abscess and fistulae, US, CT, and MRI have high and comparable accuracy. Cumulative exposure and a risk of developing a malignancy should be constantly estimated for each CD and UC patient. Numerous studies have demonstrated a considerable role of CT in the accumulated ionising dose, being responsible for more than 70% of total diagnostic medical radiation exposure [4]. The use of non-ionising examinations, like MRI and US, to alternate the radiation imaging techniques, is a reasonable option in IBD patients, who have to endure repeated diagnostic procedures.
Conclusions
The use of radiological techniques, as a completion of endoscopy, is essential for the establishment and confirmation of IBD diagnosis as well as distinction between CD and UC. Imaging modalities, like CTE, MRE, or US, enable classification of IBD and demonstrate disease activity and location. They are also required in monitoring of medical treatment and follow-up as well as assessment of complications and extraintestinal manifestations, invisible in endoscopic techniques. Finally, they can be performed when endoscopy is contraindicated or poorly tolerated. The choice of the most convenient diagnostic method should be based on the availability of the examination, the tolerance and acceptance of the procedure itself, as well as the preparation required.










