
Introduction
Diabetes mellitus (DM) is a metabolic disorder caused by insulin deficiency. Type 1 diabetes mellitus (T1DM) is an autoimmune condition characterized by T-cell-mediated destruction of pancreatic β-cells, resulting in insulin deficiency. It accounts for 10% of diabetes cases globally, with ~15,000 annual diagnoses in American youth [1, 2].
Incidence rises by 2–5% yearly, peaking at ages 5–7 and puberty. No socioeconomic correlation exists, but ethnic disparities persist. Classical symptoms of DM may include polyuria, polydipsia, weight loss, fatigue, and candidiasis. Severe insulin deficiency causes ketosis, progressing to diabetic ketoacidosis (DKA) [3, 4]. Diabetic ketoacidosis occurs in 3% of new T1DM diagnoses in the U.S., with a mortality rate of 0.15–0.31% [5].
In Iraq, delayed diagnosis contributes to a high incidence of DKA, especially in newly diagnosed T1DM [6]. Diabetic ketoacidosis arises from insulin deficiency and elevated counterregulatory hormones (glucagon, cortisol), leading to hyperglycemia, lipolysis, and ketogenesis. Osmotic diuresis then causes dehydration, electrolyte loss, and metabolic acidosis [7, 8]. DKA-induced hypovolemia reduces renal perfusion, causing pre-renal acute kidney injury (AKI), and accounts for 64% of DKA hospitalizations [9]. Persistent ischemia leads to tubular necrosis and sterile pyuria. Sterile pyuria (≥ 10 WBC/mm3) occurs in 16% of DKA cases due to systemic inflammation, not an infection. However, the distinction between sterile pyuria and true urinary tract infection (UTI) remains poorly defined [10, 11].
The pathogenesis of sterile pyuria may involve renal tubular injury, inflammatory cytokines, and systemic immune activation [12].
Recognizing whether pyuria indicates true infection or sterile inflammation is essential to avoid unnecessary antibiotic therapy and reduce healthcare burdens.
The study aimed to assess the frequency of pyuria, its microbiological relevance, and clinical implications in pediatric patients with DKA.
Material and methods
The prospective study included 150 pediatric T1DM patients (≤ 14 years) with DKA admitted to the Children Welfare Teaching Hospital between February and October 2024.
Children with T1DM meeting DKA criteria (hyperglycemia > 200 mg/dl, venous pH < 7.3, bicarbonate < 15 mEq/l, ketonuria) were included based on the guidelines of the International Society for Pediatric and Adolescent Diabetes [13].
Exclusion criteria included: age > 14 years, patients with genitourinary/chronic renal diseases such as nephrotic syndrome, glomerulonephritis, IgA nephropathy, congenital renal agenesis, renal dysplasia, as well as cases with missing data.
The patients were evaluated using;
Clinical assessment: History (demographics, symptoms, DM duration), physical examination (vitals, growth parameters, dehydration grade: mild [3–5%], moderate [6–10%], severe [> 10%]) [14].
Urine collection method for laboratory investigation: Clean catch mid-stream urine sample in most of the patients (91%), except some patients with disturbed consciousness or severe weakness, in which cases we used a urethral catheter sample (9%).
Pyuria definition: Clean catch mid-stream sample: urinalysis (pyuria ≥ 5 WBC/high-power field [HPF]: mild [5–9], moderate [10–24], severe [≥ 25]) on a centrifuged urine microscopic examination and ≥ 10 WBC/HPF in a catheterized urine specimen [12].
Urine culture method: A sterile urine sample was collected, then inoculated onto culture media (blood agar or MacConkey agar) using a calibrated loop. The plates were incubated at 35–37°C for 18–24 hours. Colony counts help determine significance: ≥ 105 CFU/ml usually indicates infection [12].
Laboratory tests: Blood glucose, arterial blood gases (ABG) (pH, bicarbonate), renal function test (RFT).
DKA severity: Mild (pH < 7.3, HCO3 < 15), moderate (pH < 7.2, HCO3 < 10), severe (pH < 7.1, HCO3 < 5) [15].
Acute kidney injury definition: According to the KDIGO (Kidney Disease: Improving Global Outcomes) criteria, AKI was diagnosed if any of the following occurred:
Increase in serum creatinine (SCr) by ≥ 0.3 mg/dl (≥ 26.5 µmol/l) within 48 hours, or
Increase in SCr to ≥ 1.5 times baseline, known or presumed to have occurred within the prior 7 days, or
Urine volume < 0.5 ml/kg/h for 6 hours [16].
Baseline creatinine was calculated via the Schwartz formula (eGFR = 0.55 × height [cm]/creatinine [mg/d]) [17].
Statistical analysis
Data were analyzed using SPSS v26 and Microsoft Excel. Categorical variables were expressed as frequency and percentage, continuous variables as mean ±SD. Tests: Kolmogorov-Smirnov (normality), χ2/Fisher’s exact (qualitative), t-test (quantitative). Significance was set at p <0.05.
Sampling power was estimated using OpenEpi, an online calculator, and a validated tool for epidemiological studies comparing 2-independent groups (with and without pyuria). Accordingly, a minimum sample size of 63 cases, totaling ~ 126 cases, was needed to achieve sufficient statistical power [18].
Results
Demographics, frequencies of pre-existing and newly diagnosed T1DM, and clinical presentation for the enrolled pediatric patients are shown in Table I.
Table I
Demographics of the study sample
The mean age of the participants was 9.16; females predominate in the study sample, with 61%, and 73% of the cases had pre-existing T1DM. The most frequently reported symptoms were nausea, vomiting, and abdominal pain, with an incidence of 78.66% and 65.33%, respectively. Regarding laboratory investigations, 84% of the cases had no urine culture performed, and 14% of the cultures were reported as positive. The mean first random blood glucose level was 395.27 mg/dl with a mean white blood cell count of 15.40 × 109/l.
It was found that 60% of the study sample had mild pyuria, 27% had moderate pyuria, and 13% severe pyuria. The remaining laboratory test results are presented in Table II. The number of DKA patients with pyuria increased gradually with time during the first 12 hours from admission (23.33% to 32.0%), as presented in Table III.
Table II
Laboratory investigations in the study sample
Table III
Timing of pyuria in the study sample
| Time | Pyuria | No pyuria |
|---|---|---|
| At admission, n (%) | 35 (23.33) | 13 (8.66) |
| After 6 hours, n (%) | 44 (29.33) | 4 (2.66) |
| After 12 hours, n (%) | 48 (32.00) | 0 (0) |
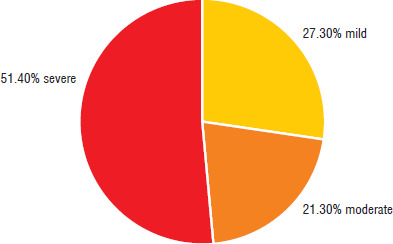
The DKA grades in the study sample are shown in Fig. 1; 51.40% had severe DKA, followed by 27.30% and 21.30% for mild and moderate degrees, respectively. The study sample was subcategorized into pyuria cases (n = 63) and cases without pyuria (n = 87).
Upon comparison, children with pyuria were significantly older (9.92 years vs. 8.61 years, p-value 0.02). Also, there was a significantly lower proportion of males (20.6% vs. 51.7%, p-value < 0.001). Moreover, mean random sugar and partial pressure of oxygen were significantly lower in the pyuria arm (370.80 mg/dl vs. 412.98 mg/dl, p-value 0.03, and 64.67 mmHg vs. 79.41 mmHg, p-value 0.009, respectively).
The frequency of weight loss was significantly higher in the pyuria arm (14.3% vs 3.4%, p = 0.01). Additionally, urine cultures were more frequently ordered for them (30% vs 5.7%, p-value less than 0.001). It was noted that all patients with positive urine culture had signs and symptoms of UTI. Other parameters were not significantly different between the study arms, as shown in Table IV and V.
Table IV
Comparison of demographic and clinical parameters between pyuria and no pyuria arms
Table V
Comparison of laboratory parameters between pyuria and no pyuria arms
Discussion
The current study enrolled 150 pediatric patients who presented with DKA to evaluate the correlation of pyuria with other clinical and biochemical parameters.
The mean age of children in the current study sample was 9.16 years, compared to an age range of 5 to 14 years among American children [19] and a mean age of 8.5 years for Ethiopian children with DKA T1DM [20].
An earlier Iraqi study by Hassoon et al. [21] found that 43.5% of children with DKA were older than 5 years and younger than 10 years. We observed predominantly female gender among enrolled cases (61% female), in line with Hassoon et al., 59.42% of whose cases were female [21]. Moreover, an Indonesian study showed female dominance at 69% [22].
The gender effect is inconsistent in the literature; Meseret et al. reported no impact of gender on DKA incidence [23], while others have reported higher incidence among the male population. This could be attributed to racial, ethnic, and study methodology differences.
Diabetic ketoacidosis was the initial presentation of newly diagnosed T1DM with an incidence of 26.67%. This figure shows wide diversity in other research, ranging from 25% to 80% of cases [24].
The most common symptoms in children with DKA were nausea and vomiting (78.66%) and abdominal pain (65.33%). This was in agreement with Satti et al. in Saudi Arabia, with incidence rates of 71.3% and 66.3% of cases, respectively [25].
Analysis showed that 42% of the children had pyuria in at least one urinalysis. The incidence of pyuria in children with DKA has not yet been identified, as this topic has not been well studied previously. The only study in the literature that assessed pyuria in the context of pediatric DKA in the United States is by Glaser et al. [12]. Their randomized controlled trial enrolled 561 children with DKA, reporting pyuria incidence of 19% in children with at least one urinalysis and 40% in those with three or more urinalyses. This incidence is almost comparable to what was reported in our study.
The high prevalence of pyuria in female patients with DKA may be attributed to many factors, including the fact that female patients are more susceptible to urethral and vaginal infection with microbes or candidiasis because of anatomical differences, in addition to other factors such as inflammation, dehydration, chemical irritation, or vaginal contamination [26].
The current analysis showed that only 3 out of 19 patients with pyuria demonstrated positive urine cultures. Similarly, Glaser et al. found that out of 17 urine cultures conducted for patients with pyuria, none had positive urine cultures [12].
Naeem et al.’s study highlighted a low positivity rate of urine culture in children presenting with DKA. They emphasized the importance of clinical judgment and considering the patient’s condition before proceeding with unnecessary tests [27].
These results might point to a non-infectious inflammatory response in the urinary tract rather than urinary tract infections, especially in asymptomatic cases [12]. Pyuria, in the context of DKA, may subject patients to unnecessary testing (urinalyses and urine cultures) and potential overtreatment. The indiscriminate use of antibiotics in DKA cases can pose a risk since AKI is associated with DKA [28]. The addition of nephrotoxic antibiotics without a solid indication can exacerbate renal injury and worsen already stressed kidneys, thus delaying recovery [29].
Type 1 diabetes mellitus is an autoimmune disease [30] in which inflammation plays a key role in both the onset and complications [31]. A retrospective study enrolled 186 pediatric patients with newly diagnosed T1DM, linking a systematic inflammatory response with DKA and its severity [32]. Although the inflammatory pathway in DKA is poorly understood, evidence suggests an association with elevated inflammatory biomarkers, including increased peripheral T-cells, elevated serum concentrations of C-reactive protein and pro-inflammatory cytokines, and activation of the complement cascade [33–34].
Pyuria in this context may reflect renal inflammation secondary to DKA rather than infection [12, 35].
The progressive increase in pyuria observed over the first 12 hours of DKA management suggests that pyuria may be a dynamic finding, potentially related to dehydration, urinary ketone excretion, or catheterization. Therefore, pyuria should be interpreted cautiously, and urine cultures should be obtained to confirm true urinary tract infections, avoiding unnecessary antibiotic use. However, the high prevalence of mild pyuria in this setting may reflect local urethral infection or inflammation [12, 32].
In the current study, AKI incidence was 2.67%, which was notably lower than previously reported rates, which ranged from 10 to 64% in general pediatric wards and up to 80% in ICU settings [36].
Alyahyawi’s study noted that AKI risk was higher among severe DKA cases requiring ICU admittance, and the AKI rates were affected by the setting and DKA severity [37].
A possible explanation for the disparity between our results and those of others is the earlier presentation of DKA cases and timely management. Finally, the sample size may have been a contributing factor that obscured the true incidence of AKI.
Study limitations
A multicentric study with larger sampling power and a longitudinal design may have performed better. A longitudinal study with extended follow-up is recommended to fully characterize the relationship of pyuria with DKA and its clinical outcomes. We did not include inflammatory biomarkers for renal injury, which may have strengthened the link between pyuria and renal inflammation. Additionally, not all patients in our study underwent urine culture, because the test was not available outside the hospital’s official working hours.
Study strengths
This prospective study focused on important clinical scenarios regarding the significance of pyuria among pediatric DKA cases: it highlights that pyuria in pediatric DKA only reflects renal inflammation rather than UTI, particularly among asymptomatic cases. It supports more selective use of urine cultures and antibiotics, promoting diagnostic precision and reducing unjustified medical intervention. Our results contribute to improving clinical decision-making in pediatric DKA management.
Conclusions
Pyuria is a common finding among pediatric patients with DKA, yet it rarely signifies a true UTI. Its clinical relevance in this setting remains uncertain, with limited evidence supporting a consistent correlation with patients’ clinical or biochemical parameters. Routine antibiotic therapy based solely on pyuria is not recommended without supporting clinical or microbiological evidence, as it may lead to unnecessary treatment. For this, clinical judgment should guide the decision regarding urine testing and antibiotic intake, which should be reserved for DKA cases with clear UTI features to avoid unnecessary interventions and optimize patient care.









